Regenerative Medicine
Clinical insights by Prof. Dr. Erdinç Civelek
When patients come in with lower back pain, they often use these two phrases as if they mean the same thing.
“I have disc disease.”
“I have a herniated disc.”
Sometimes they were told one.
Sometimes the MRI report mentioned the other.
Sometimes both appear in the same conversation, and the patient leaves thinking they are just two names for one problem.
They are not.
They are related, yes. Very often they overlap. But they are not the same. And this makes a big difference. Bigger, than most patients think.
Because once you mix them together, everything else becomes confusing too.
Why the pain feels different.
Why one patient mainly has lower back pain while another has leg pain.
Why one patient may improve with time while another needs faster intervention.
Why a regenerative treatment discussion may make sense in one case and not in another.
So the question is not only, “Which one do I have?”
The better question is:
“What exactly is happening to the disc?”
A lumbar disc is supposed to absorb load, support movement, and act like a cushion between the vertebrae.
Over time, that disc can begin to change.
It may lose water.
It may lose elasticity.
Small cracks may form.
The internal structure becomes weaker.
The intervertebral disc can flatten, dry out or lose its elasticity.
When this happens, doctors generally refer to a disc disorder, or, to use the medical term, degenerative disc disease of the lumbar spine.
This process is described in similar terms in specialist texts. Here, the focus is on a change in cell function combined with a breakdown of the matrix. This then automatically leads to a change in the mechanics of the intervertebral disc.
Patients usually notice it before they know the term.
They say the back feels stiff.
Or weak.
Or unreliable.
Sometimes it is not dramatic pain at all. Just the sense that the lower back is not behaving like it used to.
That is often how it begins.
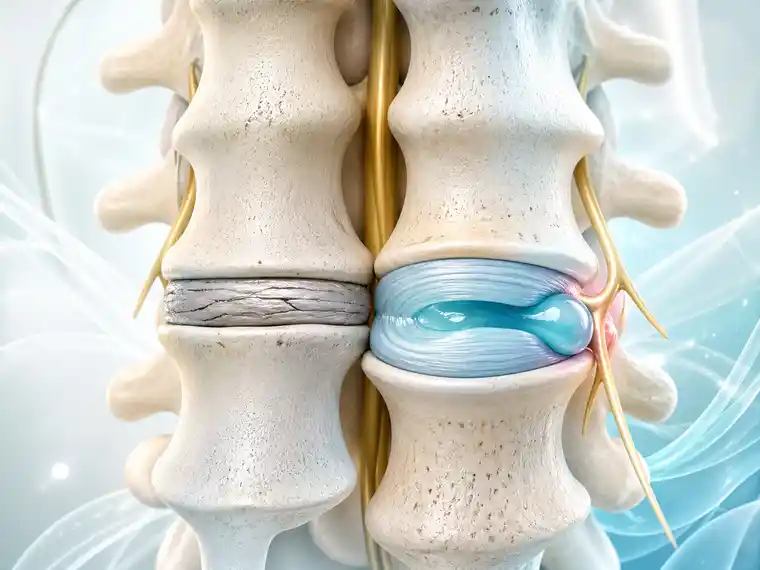
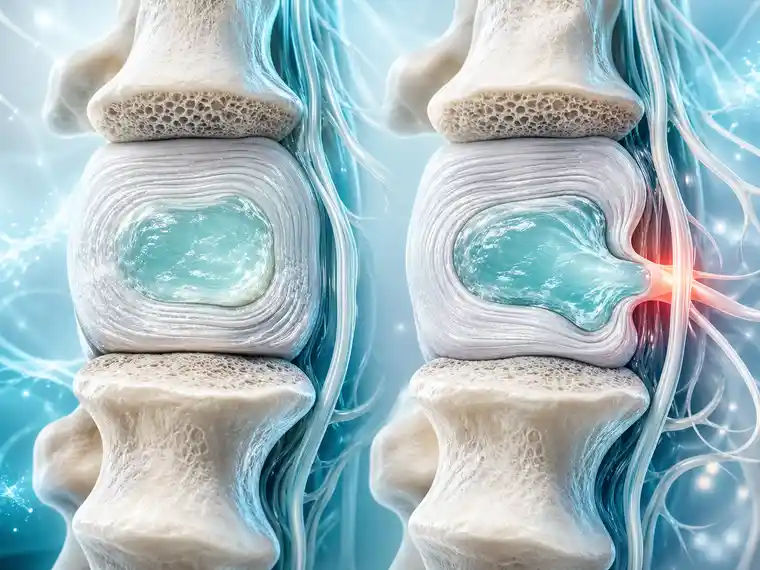
A herniated disc is more specific.
It means disc material has pushed out beyond where it should normally remain. That can happen through a weakened or torn outer ring of the disc, and depending on the shape and size of the herniation, the disc may irritate or compress nearby nerve structures. Reviews of lumbar disc herniation describe it as a distinct disc pathology that can produce both local lower back pain and radicular leg symptoms.
In simple terms:
Lumbar disc disease is the broader degenerative process.
A herniated disc is one specific event or structural problem that can happen within that process.
That is why one can exist without the other.
A patient may have lumbar disc degeneration without a true herniation.
A patient may also have a herniated disc on top of an already degenerating disc.
And that is where the confusion usually begins.
The shortest answer is this:
Lumbar disc disease describes the disc wearing down over time.
A herniated disc describes disc material pushing outward in a more focal way.
That may sound simple, but clinically it changes a lot.
Disc disease often behaves like a chronic quality problem.
A herniation often behaves like a focal structural problem.
Disc disease may be more likely to produce:
A herniated disc is more likely to produce:
Of course, real patients are not textbooks.
Many people have both.
This is where patients often get frustrated.
They hear “disc problem” and expect one clear symptom pattern.
But discs do not create problems in only one way.
A degenerated lumbar disc may hurt because the disc itself has become painful.
A herniated disc may hurt because the nerve is inflamed.
It may also hurt because the nerve is physically compressed.
And sometimes both things are happening at once.
That is why one patient has mostly lower back pain, while another has sciatica.
That is also why MRI language can be misleading if it is read too literally.
A scan may show degeneration.
Or bulging.
Or protrusion.
Or extrusion.
Or sequestration.
But the image itself does not automatically tell you which finding is actually causing the pain. Disc degeneration and herniation are both common imaging findings, and symptoms depend on the clinical context, not the report alone.
Yes, often it can.
A degenerating disc becomes weaker and less resilient over time. When the disc dries out, loses elasticity, and develops annular damage, it can become more vulnerable to bulging or herniation. Reviews of degenerative disc disease describe this loss of proteoglycans, hydration, and structural integrity as part of the degenerative cascade that increases susceptibility to further disc injury.
So in real life, these two problems often belong to the same story.
Not always.
But often.
That is why many patients are told they have both disc degeneration and a herniated disc in the lower back.

Usually the herniated disc is the more obvious suspect when the pain shoots into the leg.
That is because radicular symptoms usually mean a nerve root is being irritated, inflamed, or compressed. Lumbar disc herniation is a classic cause of sciatica and radiculopathy.
That said, real cases are not always perfectly clean.
A patient can have lumbar disc disease, annular injury, inflammation, and a herniation all contributing together.
So when patients ask,
“Is it the degeneration or the herniation causing my pain?”
the honest answer is sometimes:
“Probably both, but not equally.”
That is why examination still matters.
And symptom pattern matters.
And imaging must be interpreted, not just read.
Patients often ask this directly.
There is no universal answer.
A mild herniated disc may settle.
A badly degenerated disc may create long-term lower back pain for years.
A large lower back herniated disc with major nerve compression may become more urgent than ordinary disc degeneration.
A chronically painful disc without dramatic herniation can still be life-changing in terms of function and quality of life.
So “more serious” depends on what the disc is doing.
If the main issue is chronic disc-related lower back pain, lumbar disc disease may be the central problem.
If the main issue is nerve compression, weakness, or significant sciatica, the herniation may be the more pressing issue.
That is why the name alone never tells the full story.
This is where patients really need clarity.
Because treatment logic changes depending on what the real problem is.
If the issue is mainly lumbar disc disease, the discussion often focuses on:
If the issue is mainly a herniated disc, the discussion may focus more on:
That does not mean the two treatment paths are completely separate.
It means the priority changes.
And that is exactly why it is not enough to say only:
“I have a disc problem.”
MRI wording creates a lot of unnecessary fear.
Patients read:
and understandably think the whole spine is collapsing.
Usually it is not that simple.
Degenerative findings are common.
Some herniations are clinically important.
Some are not.
Some look dramatic on MRI and settle with time.
Others look modest but create intense symptoms because of where they are touching the nerve.
So the MRI matters.
But it does not speak alone.
The better question is never just:
“What does the scan say?”
It is:
“Does the scan match the pain pattern, the examination, and the actual patient in front of us?”
Most lower back disc problems are not emergencies.
But some situations are more serious and should not be minimized.
Faster evaluation matters if there is:
Those are not situations for casual internet interpretation.
And they should definitely not be blurred by loose language about “disc disease” in general.
For many patients, the difficult part is not learning the difference between lumbar disc disease and a herniated disc. The difficult part is understanding which finding actually matters in their own case.
An MRI may describe degeneration, bulging, protrusion, or herniation. But these words only become meaningful when they are compared with the patient’s symptoms, physical examination, pain pattern, and daily limitations. Lower back pain, leg pain, numbness, or weakness may all point in different directions.
That is why a proper medical assessment can be useful before deciding on treatment. The goal is not simply to react to the most frightening word in the MRI report. It is to understand whether the main problem is disc degeneration, nerve irritation, a true herniation, or a combination of these factors.
With that clarity, the next step can be chosen more carefully — whether that means conservative care, further evaluation, regenerative treatment discussion, or surgical opinion when necessary.

No, not really. They are connected, but they are not the same diagnosis. Lumbar disc disease is the broader wear-and-change process in the disc over time. A herniated disc is more specific. It means part of the disc has pushed outward in a way that can irritate or compress a nerve. So one is the bigger background story. The other is a more defined event or structural problem within that story.
Yes, very easily. In fact, many patients do. The disc can lose water, height, and elasticity without ever producing a true herniation. Those patients may still have lower back pain, stiffness, flare-ups, or the feeling that the back is becoming weaker or less reliable. So disc disease does not automatically mean the disc has herniated.
Sometimes, yes. Not every herniated disc happens in a spine that is already badly degenerated. But very often there is still some weakness or wear in the disc tissue, even if the patient has not been told they have “disc disease” before. So the short answer is yes, but the two often overlap.
Both can do that. But they often do it a little differently. Lumbar disc disease is more often part of the chronic lower back pain picture — the kind that lingers, flares, and makes the back feel stiff or unreliable. A herniated disc can also cause lower back pain, of course, but when it becomes more specific, it often starts involving the leg as well. That is usually where the story changes.
Most of the time, the herniated disc. When the pain starts traveling down the leg, we begin thinking more seriously about the nerve. That is often the moment the picture changes. A patient who first thought, “I just have lower back pain,” suddenly says, “Now it shoots into my hip,” or “I feel it down the back of my leg.” That kind of pain pattern is much more typical when disc material is irritating the nerve root. So if the main complaint is true sciatica, a herniated disc usually moves higher on the list than disc degeneration alone.
No, not at all. This is one of the biggest misunderstandings. Many herniated discs improve without surgery. Time, inflammation reduction, movement control, and proper follow-up matter a lot. But the answer changes if there is progressive weakness, severe neurological deficit, or other red-flag findings. So no, herniated disc does not automatically mean surgery. But it also should not be minimized when the nerve symptoms are becoming more serious.
The difference between lumbar disc disease and a herniated disc is simple in theory, but in real patients it often overlaps.
That is why the right question is not only:
“What label do I have?”
The better question is:
“What is my disc actually doing?”
Because that is what decides the next conversation.
Not the vocabulary alone.
Not the MRI word that sounds scariest.
And not whichever phrase the patient happened to hear first.
A disc can degenerate.
A disc can herniate.
Sometimes it does both.
Good spine care begins when those two things stop being treated as if they are identical.