Clinical insights by Prof. Dr. Erdinç Civelek
How to decide: Lumbar Disc Disease Surgery or Not?
When patients hear the words lumbar disc disease, many of them immediately split into two camps.
One is afraid of surgery from the first minute.
The other is already asking for it.
Usually both reactions come too early.
Because the real question is not:
“Do I have lumbar disc disease?”
The real question is:
“What is the disc actually doing, and is surgery solving the right problem?”
That distinction matters.
Some patients have lower back pain from a disc that has dried out, weakened, and become chronically painful. Others have a lower back disc problem that is no longer just painful, but mechanically disruptive. And then there are the patients with a herniated disc, nerve compression, sciatica, weakness, or symptoms that are no longer behaving like something that will simply settle with time. Those are not the same conversations, even if they all begin with the same MRI word: disc.
So yes, lumbar disc disease does not automatically mean surgery.
But it also does not mean surgery is never needed.
Table of Contents
When Lumbar Disc Disease Becomes More Than Wear and Tear
Patients are often told that disc degeneration is just part of aging.
That is not entirely wrong.
But it is also not enough.
A lumbar disc can lose water, elasticity, and structural integrity over time. It can flatten. Crack. Become less resilient. The disc environment changes biologically and mechanically. That is the process behind lumbar degenerative disc disease. But the important part is not the definition. The important part is what that degeneration is doing in real life.
Some discs look worn on MRI and cause very little trouble.
Some cause chronic lower back pain for years.
Some become part of a more urgent picture because degeneration is no longer the whole story. Now there is nerve irritation, herniation, motor weakness, or instability of function.
That is where surgery enters the discussion.
Not because the MRI looks ugly.
Because the clinical situation changes.
Surgery Is Not the First Answer in Most Cases

This is worth saying clearly.
Most patients with lumbar disc problems do not go straight to surgery.
For symptomatic lumbar disc herniation, symptoms improve in about 60 to 80 percent of patients within 6 to 12 weeks, and in 80 to 90 percent over the longer term. In the absence of major neurologic deficits, I generally support a period of conservative treatment first.
That means many patients do well with:
- time,
- movement guidance,
- physical therapy,
- pain control,
- inflammation management,
- and careful follow-up.
So when a patient asks,
“Do I need surgery because I have lumbar disc disease?”
the honest answer is often:
“Not necessarily.”
And sometimes:
“Not even close.”
When Surgery Starts to Become More Reasonable
The conversation changes when the symptoms stop behaving like an ordinary flare.
Surgery becomes more relevant when there is:
- clear nerve-root compression with persistent leg pain,
- worsening neurological deficit,
- progressive weakness,
- severe sciatica that does not settle despite proper treatment,
- or a structural problem that continues to match the symptoms over time.
That does not mean every patient needs emergency surgery the moment leg pain appears.
But it does mean we start listening differently.
Because lumbar disc disease is one thing.
Lumbar disc disease with significant nerve compression is another.
And once weakness enters the picture, the discussion is no longer only about comfort.
It becomes a function question too.
When Lumbar Disc Disease Still Needs Surgery Despite “Trying Everything Else”
This is where many patients arrive emotionally exhausted.
They have already:
- tried medication,
- tried physical therapy,
- tried rest,
- tried injections,
- tried waiting,
- tried being careful,
- and still the lower back pain or nerve pain keeps taking over daily life.
At that point, the question becomes more practical.
Not:
“Can I tolerate this?”
But:
“Is there still a realistic non-surgical path here?”
If a patient has had an adequate course of conservative treatment and still has persistent intolerable symptoms that match the imaging and examination, then surgery may become a reasonable next step. Experince has shown, that a 6-to-12-week conservative period as appropriate in many non-emergency lumbar disc herniation cases before surgery is considered, assuming there is no major neurological deterioration.
That is not a rigid stopwatch.
It is a clinical pattern.
Some patients improve early and avoid surgery.
Some do not.
And some show you quite clearly that waiting longer is not helping.
When Surgery Becomes Urgent
This part should never be softened.
Some lumbar disc cases are not just “still painful.”
They are urgent.
Cauda equina syndrome, including bladder or bowel dysfunction caused by lumbar disc herniation, is widely treated as a surgical emergency that requires immediate decompression, generally within 24 to 48 hours. Significant or rapidly progressive neurological deficits are also treated much more urgently than ordinary pain alone.
So if a patient has:
- new bladder or bowel dysfunction,
- saddle numbness,
- rapidly worsening weakness,
- or major neurological decline,
that is not the time to “see how it goes for another few weeks.”
Those are the cases where surgery is no longer a lifestyle preference.
It becomes a protective decision.
Lower Back Pain Alone Is Not Always a Surgical Problem
This is another point patients deserve to hear clearly.
Chronic lower back pain by itself does not automatically point toward surgery.
That is where many people get disappointed.
They assume:
“Pain is severe. MRI shows degeneration. So surgery must fix it.”
But spine decision-making is not that simple.
Pain can come from:
- disc degeneration,
- annular injury,
- muscle guarding,
- facet changes,
- inflammation,
- nerve irritation,
- and sometimes several things at once.
So the presence of lower back pain alone is not enough.
The question is whether the pain pattern, the structural finding, and the functional limitation all line up strongly enough to support a surgical target.
If they do not, surgery may not help in the way the patient imagines.
And that is exactly why the better surgeons are usually the ones who are careful.
Herniated Disc vs Lumbar Disc Disease: Why the Surgery Decision Is Different
Patients often mix these two together.
That causes a lot of confusion.
A chronically degenerating disc may produce lower back pain, stiffness, and loss of function over time.
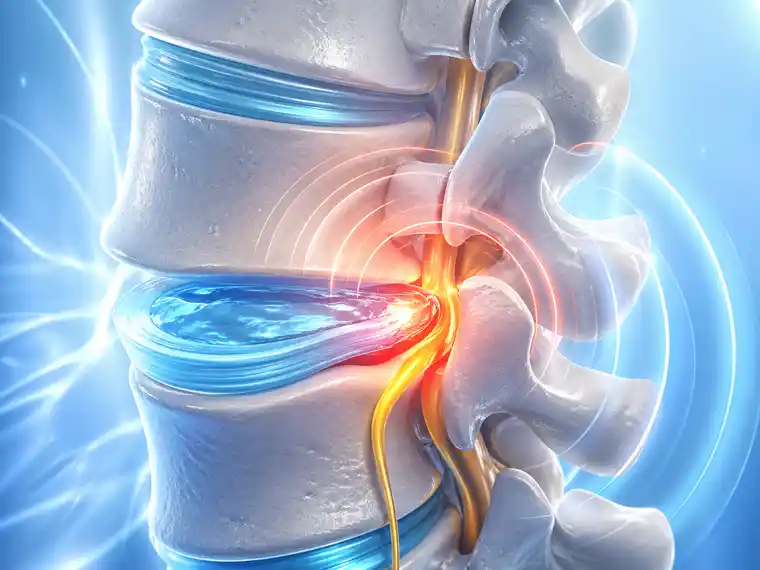
A herniated disc is more likely to create focal nerve compression, sciatica, and neurologic symptoms.
Those are not identical treatment decisions.
A patient with lumbar disc disease but no meaningful nerve compression may still be very symptomatic, but the surgery discussion is usually more cautious.
A patient with a lower back herniated disc and progressive weakness may enter the surgery conversation much faster.
That is why the question is never just:
“Do I have disc disease?”
It is:
“What exactly is this disc doing?”
What Surgery Is Actually Trying to Solve
Patients sometimes picture surgery as a general reset button.
It is not.
Surgery works best when the target is clear.
In lumbar disc herniation, the goal is usually decompression:
remove the disc fragment, free the nerve, reduce the mechanical irritation. Modern reviews describe microsurgical and endoscopic decompression as standard approaches, with the main aim being safe removal of the offending disc material and relief of nerve compression.
That is different from a looser idea like,
“My whole lower back is bad.”
Surgery is strongest when it is solving a defined structural problem.
The less defined the problem, the more careful the decision should be.
When Not Having Surgery May Still Be the Better Decision
This part matters just as much.
Sometimes the disc looks bad.
The patient feels awful.
And surgery is still not the best next step.
That happens when:
- symptoms are improving,
- there is no meaningful neurological loss,
- the pain pattern does not clearly match the imaging,
- the lower back pain is broad and nonspecific,
- or the patient has not yet had a fair conservative trial.
That is not neglect.
That is proper patient selection.
The goal is not to operate on the worst-looking MRI.
The goal is to operate on the right problem.
FAQs About When Lumbar Disc Disease Still Needs Surgery
Does lumbar disc disease always need surgery?
No, usually not. This is one of the first fears many patients have after reading an MRI report. They see words like degeneration or disc disease and immediately think surgery must be somewhere around the corner. But that is often not the case. Many lower back disc problems are managed without an operation, especially when there is no progressive weakness, no major neurological loss, and no urgent warning sign. So the important question is not simply whether disc disease is present. It is whether that disc problem has actually reached a point where surgery is solving something that other treatment no longer can.
When does surgery start to become more likely?
Usually when the back — or the leg — keeps showing you that it is not settling. A patient may wait a few weeks and still say, “It is just as bad.” Or worse: “Now I cannot trust my leg.” That is usually the moment the tone changes. Not because surgery suddenly becomes attractive. Because the problem stops looking temporary. If the pain keeps taking over daily life, if the leg symptoms stay strong, if weakness starts to appear, or if the patient is functioning less instead of more, then waiting may no longer be the smart part of the plan. That is often when surgery moves from being a distant option to a real discussion.
Is lower back pain by itself enough to need surgery?
Usually not. This is one of the biggest misunderstandings in spine care. A patient can have strong lower back pain and still not have a good surgical target. Pain alone is not always the deciding factor. What matters is whether the symptoms, the examination, and the imaging all point clearly to a structural problem that surgery can actually address. Sometimes they do. Sometimes they really do not. And that difference matters more than the pain intensity by itself.
Does a herniated disc usually lead to surgery faster than ordinary disc degeneration?
Very often, yes. Not automatically. But more often. The reason is simple: once a herniated disc starts irritating or compressing a nerve, the situation changes. Now we are not talking only about a worn disc. We may be talking about sciatica, neurological symptoms, loss of strength, or a pain pattern that is much more clearly connected to one specific structure. That usually makes the surgical discussion more focused.
When does it become urgent?
When the symptoms stop being ordinary pain symptoms and start looking more like neurological danger signs. That means things like new bladder or bowel problems, saddle numbness, rapidly worsening weakness, or major loss of control in the leg. Those are not the kinds of symptoms patients should sit with at home and keep observing for another few weeks. That is the point where the timing matters much more.
How long should someone usually try conservative treatment first?
There is no magical number that fits every patient, but in many non-emergency cases, patients are first given time for the problem to settle with proper conservative treatment. That often means a period of weeks rather than days. But the real answer depends on what the symptoms are doing. If the pain is easing, strength is stable, and the patient is improving, the lower back may still be on a reasonable non-surgical path. If the opposite is happening, the timeline starts to matter differently. So the clock is never the only decision-maker. The patient’s actual course matters more.
Final Thoughts
Lumbar disc disease does not automatically need surgery.
But it can still reach that point.
The decision changes when the disc problem is no longer just present on MRI, but is clearly driving persistent symptoms, nerve dysfunction, or loss of function in a way that conservative treatment is no longer solving.
That is usually where the real answer lives.
Not in fear.
Not in impatience.
And not in the word degeneration alone.
But in the actual behavior of the lower back problem, the neurological picture, and whether surgery is treating a real target instead of a general frustration.
When a Back Check Makes Sense
Back pain can be hard to read. Sometimes the disc looks bad, but surgery is not the right step. Sometimes the symptoms are more serious than the patient first thought.
So it makes sense to check properly before deciding. Look at the MRI. Look at the leg symptoms. Talk about weakness, numbness, pain, and what has already been tried. Then it becomes easier to say whether surgery should really be discussed, or whether another treatment path makes more sense.