Regenerative Medicine
Clinical insights by Prof. Dr. Erdinç Civelek
When patients come in with lower back disc problems, they usually do not start with the phrase “lumbar degenerative disc disease.”
They say something more direct.
“My disc is worn out.”
“I have a herniated disc in the lower back.”
“The pain keeps coming back.”
Or: “Is there anything besides surgery and painkillers?”
That is the real starting point.
Because in daily practice, lumbar disc degeneration is not one neat diagnosis with one neat answer. One patient has chronic disc-related back pain with a dried, collapsed disc. Another has a lower back disc herniation irritating a nerve. Another has both: degeneration in the disc itself and an acute or recurring herniation on top of it. Those problems can belong to the same broader process, but they do not behave in exactly the same way.
That matters.
Stem cell and exosome therapy entered this conversation because standard treatment does not always solve the biological side of the problem. Medication may reduce pain. Physical therapy may improve function. Injections may calm inflammation for a while. Surgery may be the right answer in selected cases, especially when compression is severe. But none of that automatically means the disc itself has recovered. That is why regenerative treatment became interesting in the first place.
The question is not whether the lower back hurts.
The better question is what, exactly, is causing that pain — and whether the part we are trying to treat is mainly mechanical, mainly biological, or both.
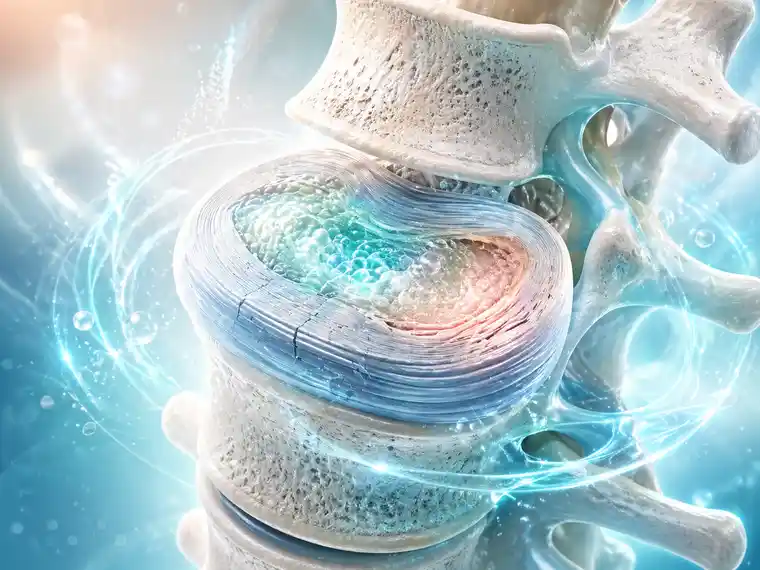
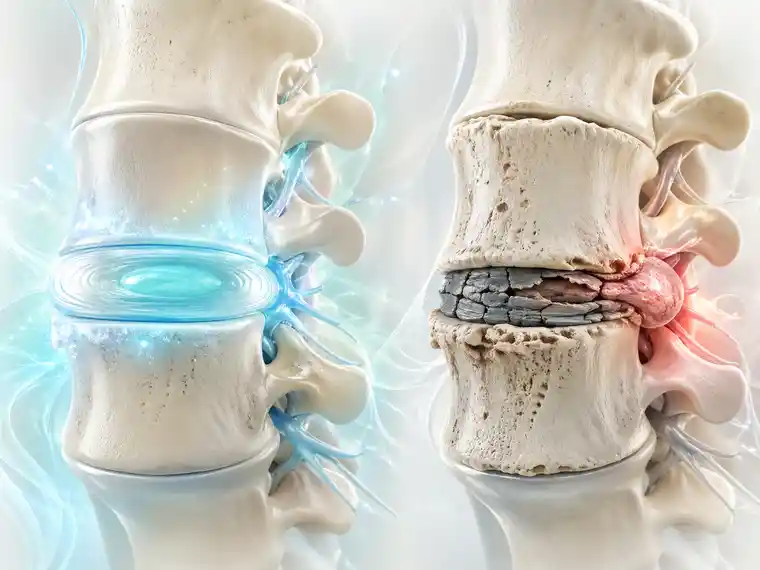
A healthy lumbar disc is built to absorb load, distribute pressure, and allow movement. Over time, this intervertebral disc can lose moisture and its structure becomes softer, so to speak. The quality of the matrix changes. When the disc loses moisture, it automatically loses its elasticity – just as happens with all things when they dry out. Cracks then begin to form. Just imagine it like soil in a flower pot that slowly dries out and eventually cracks. Naturally, this causes pain in humans. Furthermore, ‘dried-out’ intervertebral discs are more prone to herniation.
So you see, degenerative disc disease in the lower back is not simply a matter of ‘wear and tear’ that just happens over the years.
Patients usually feel that long before they use the textbook words.
They tell you the back feels weak.
Or always tight.
Or unreliable.
Sometimes the pain stays in the lower back. Sometimes it shoots into the leg. Sometimes the MRI report says degeneration, protrusion, annular tear, or herniation, and the patient is left trying to understand whether all of those words mean the same thing.
They do not.
A painful degenerated disc without major nerve compression is one conversation.
A contained herniation is another.
A large lower back disc herniation pressing hard on a nerve root is another again.
That is exactly why regenerative treatment cannot be discussed as if every disc problem belongs in the same category.
Stem cell therapy is being studied in disc degeneration because researchers are trying to influence the disc environment itself.
Not cosmetically.
Not symbolically.
Biologically.
Mesenchymal stem cell approaches are of interest because they may help modulate inflammation, support matrix-related repair pathways, influence cell survival, and possibly improve the environment inside a degenerated disc. Reviews and meta-analyses in this field describe encouraging signals for pain and function in selected patients, but they also make clear that the evidence is still limited by small studies, mixed protocols, and lack of standardization.
And there is another problem patients rarely hear explained properly:
A degenerated lumbar disc is a difficult place to heal.
It is not richly vascularized tissue. It is a hostile environment. Low oxygen, altered acidity, chronic stress, inflammatory signaling, and mechanical loading all make regeneration harder than many advertisements suggest. That does not mean stem cells are irrelevant. It means the biological idea is serious, but the setting is unforgiving.
So if a patient asks, “Can stem cells regenerate a damaged lumbar disc?” the honest answer is not yes or no.
It is: possibly, in selected cases, but not in the simplistic way many people imagine.
Exosomes are being studied for a related reason, but they are not the same thing as stem cells.
They are tiny extracellular vesicles released by cells. What makes them interesting is not that they are fashionable. It is that they carry signals — the kind of signals researchers believe may influence inflammation, tissue response, apoptosis, and repair pathways inside the disc. In intervertebral disc degeneration research, exosomes are being explored as a cell-free regenerative strategy, which is one reason the field has moved so quickly in recent years.
That sounds attractive, and understandably so.
Patients hear “cell-free” and often assume that means simpler, safer, or already settled. It does not. Recent reviews still emphasize very real problems with sourcing, isolation, standardization, and delivery. Most of the stronger exosome evidence in disc disease remains preclinical, not mature large-scale human outcome data.
So exosomes are not imaginary.
They are not meaningless.
But they should not be described as if the science is finished.
It is not.
Sometimes this is where the conversation becomes confusing.
Because a lower back disc herniation can hurt for different reasons.
A herniated disc may cause pain because the nerve is inflamed and chemically irritated. It may also cause pain because the disc material is physically compressing the nerve. Those are not the same problem, even though both may produce sciatica or leg pain.
That distinction matters more than people think.
Regenerative treatment may be biologically relevant when disc degeneration, inflammation, and tissue dysfunction are important parts of the picture. But if the main problem is a large lower back disc herniation producing major nerve compression, worsening weakness, or red-flag symptoms, stem cell or exosome therapy should not be presented as a substitute for urgent spine evaluation. A biological treatment does not mechanically remove a disc fragment that is already compressing a nerve root.
So yes, herniated discs belong in the discussion.
But not every herniated disc belongs in the same regenerative discussion.
That is where good clinical judgment begins.
The stem cell side of this field has early human data, and some of it is encouraging. A 2023 systematic review and meta-analysis of mesenchymal stem cells for discogenic pain found improvement signals in pain and disability outcomes, but the included studies were still limited in number and design.
That is important.
Because it means the field has moved past pure theory, but it has not reached the point where every clinic should speak with certainty.
The exosome side is even earlier. Reviews from 2024 and 2025 describe strong mechanistic interest and promising preclinical results in intervertebral disc degeneration, especially around inflammation control, apoptosis reduction, and matrix-related repair. But that is still not the same as large, standardized, long-term human proof.
So the balanced answer is this:
The science is real.
The rationale is credible.
The interest is justified.
But the evidence is still developing.
That is the line patients deserve to hear.
Usually, the more reasonable candidates are not the people looking for a miracle.
They are the patients whose actual problem fits the biology we are trying to influence.
That may include people with lumbar degenerative disc disease who have persistent disc-related pain despite appropriate conservative care. It may include selected patients with earlier or moderate degeneration rather than complete structural collapse. And it may include some patients with lower back herniated discs when inflammation, annular injury, and degenerative disc biology are meaningful parts of the picture, not just pure mechanical compression.
The better candidates usually sound like this:
“I want realistic improvement.”
“I want less pain and better function.”
“I want to understand whether this makes sense in my case.”
That mindset matters.
Because this kind of treatment discussion is usually strongest when the question is measured.
Not magical.
This is just as important.
A poor candidate may be someone with severe neurological symptoms, progressive motor weakness, or urgent red-flag findings that demand faster mechanical decision-making. It may also be someone with advanced structural collapse where the disc is already far beyond a realistic biological target. And sometimes the poor candidate is not medically unsuitable at all — just badly matched to the treatment.
That happens more often than patients realize.
If someone expects one injection to rebuild a badly failed lower back disc, that is a mismatch.
If someone expects a large herniated fragment to simply disappear because the treatment sounds advanced, that is a mismatch.
If the clinic cannot explain clearly what is being used, why it is being used, and what part of the problem it is meant to address, that is also a mismatch.
A good treatment conversation always begins with a good diagnostic conversation.
Otherwise, the label becomes more important than the logic.
And that is never a good sign.
This is where the most damage is often done online.
Not because the treatment is worthless.
Because the language becomes careless.
A realistic goal may be pain reduction, better daily function, calmer flare-ups, and improved tolerance for movement and activity. In some patients, it may also mean support for the disc environment itself, not in a dramatic cinematic way, but in a quieter biological sense.
What patients should not automatically expect is just as important.
Not every disc will regenerate.
Not every lower back herniation will respond.
Not every patient will avoid surgery.
Not every clinic offering “regenerative treatment” is offering the same thing.
That is not negativity.
That is how responsible spine medicine sounds when it is honest.
Possibly to a limited degree in selected cases, but that is not the same as growing a brand-new disc. The realistic discussion is usually about supporting the disc environment, reducing pain, and possibly improving tissue behavior — not fully restoring a severely failed lumbar disc to normal.
They may become relevant in this field because of their signaling role and their potential effects on inflammation and tissue response. But for lumbar disc disease, the stronger exosome evidence is still mostly preclinical, so they should be discussed carefully, not as a fully proven answer.
Not in every case. If a lower back herniated disc is mainly causing pain through inflammation, a regenerative discussion may make sense in selected patients. But if there is major nerve compression, progressive weakness, or urgent neurological concern, regenerative treatment should not be framed as a substitute for appropriate surgical evaluation.
At this stage, it is reasonable to say the field is trying to address both. The research interest comes from possible support for tissue repair pathways and from the hope of reducing disc-related pain. But patients should understand that these two goals do not always progress equally, and neither one should be oversold.
Usually, the better candidate is the patient whose imaging, symptoms, and examination all point in the same direction — and whose problem still has a meaningful biological target. Earlier or moderate lumbar disc degeneration with persistent symptoms is usually a stronger regenerative discussion than a spine that is already structurally devastated or neurologically urgent.
No. The science is real and the field is moving, but the evidence is still developing. Stem cell therapy has early clinical data and encouraging meta-analytic signals in selected patients. Exosome therapy has strong biologic interest and promising preclinical work, but standardization and human evidence remain limited.
Stem cell and exosome therapy for lumbar degenerative disc disease are being studied for a good reason.
They ask a better question than many older treatment models asked.
Not only, “How do we block pain?”
But also, “Can we support the damaged disc environment itself?”
That is why this field matters.
But serious medicine has to stay disciplined.
The biology is promising.
The research is meaningful.
Some patients may benefit.
But a lower back disc problem is still a mechanical problem, a biological problem, or both — and no regenerative treatment should be discussed intelligently until that balance is understood.
So if a patient asks me whether stem cell or exosome therapy may help a degenerative lumbar disc or a herniated disc in the lower back, my answer would be this:
Possibly, yes.
But only when the diagnosis is defined properly.
Only when the lower back problem fits the biology we are trying to treat.
And only when expectations stay honest from the beginning.