Clinical insights by Prof. Dr. Erdinç Civelek
Understanding Lumbar Disc Disease On MRI
When patients open an MRI report for the first time, the reaction is often the same.
They stop at one or two words and everything else disappears.
- Degeneration.
- Bulging.
- Protrusion.
- Annular tear.
- Sequestration.
And from that moment on, many of them assume the lower back is falling apart.
That is understandable.
MRI language sounds heavier than it often is.
The problem is that many patients start treating the report like a final verdict, when in reality it is only one part of the picture. An MRI is excellent for showing disc pathology and soft-tissue detail in the lumbar spine, but the findings still have to be interpreted in the context of symptoms and examination.
That difference matters.
Because one patient can have an MRI full of lumbar disc disease findings and very tolerable symptoms. Another can have a report that looks less dramatic and still feel miserable. And another can have a scan that shows several abnormalities, while only one of them is actually relevant to the pain.
So the better question is usually not:
“What bad things did the MRI find?”
It is:
“What on this MRI actually matters for my lower back problem?”
Table of Contents
When Lumbar Disc Disease Starts To Show Up On MRI
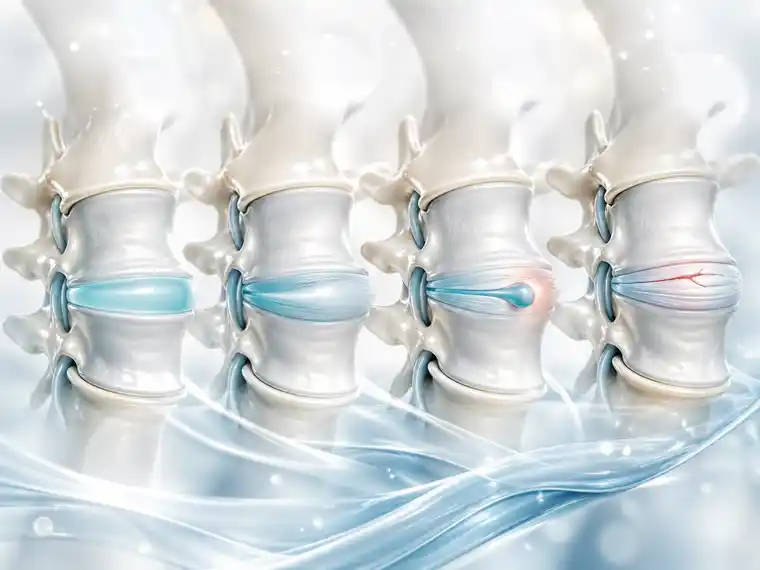
A lumbar disc changes over time.
It can lose water.
It can flatten.
Its internal structure can weaken.
Small fissures can appear.
The disc may start behaving less like a healthy cushion and more like tissue under chronic strain.
That is the broader process behind lumbar degenerative disc disease, and MRI is very good at showing those changes. Reviews and observational work describe disc degeneration on MRI in terms of disc height loss, annular tears, bulging, protrusion, extrusion, and associated narrowing around the canal or foramina.
But seeing those findings does not automatically answer the most important question:
“Is this why the patient hurts?”
That is where experience still matters more than the scan alone.
What Doctors Usually Mean By “Disc Degeneration” On MRI
Patients often read the word degeneration as if it means severe damage.
Usually it is not that simple.
On MRI, degeneration often refers to a combination of changes in the disc:
- loss of hydration,
- loss of height,
- darkening of the disc signal,
- weakening of the disc structure,
- and sometimes associated contour changes such as bulging or protrusion.
In plain language, the disc is no longer behaving like a healthy young disc.
That matters.
But it is also very common.
And that is the part patients need to hear clearly.
Lumbar degenerative findings on MRI do not always equal a major clinical problem. Some are strongly relevant. Some are incidental. Some are part of ordinary aging or long-term load. The clinical meaning depends on the whole picture, not on the word itself.
What Common MRI Terms Usually Mean
This is where most of the fear comes from, so it helps to slow it down.
Sequestration
This usually means the disc has lost water.
Patients often imagine something dramatic when they read it, but in many cases it simply reflects disc drying over time and rupting. It is one of the common MRI signs of lumbar disc degeneration.
Bulging
A disc bulging usually means the disc extends beyond its normal margin in a broader, less focal way.
It does not automatically mean the nerve is trapped.
Protrusion
A protrusion is more focal than a bulging. Disc material pushes outward, but the base is still broader than the outward extension.
Extrusion
This usually means the disc material has pushed out more significantly, often in a way that sounds more dramatic and sometimes is more clinically important, depending on where it is.
Annular Tear Or Fissure
This refers to a crack or disruption in the outer ring of the disc.
Patients often focus on that phrase because it sounds severe. Sometimes it is relevant. Sometimes it is only part of the background degenerative picture.
Nerve Root Compromise
This matters more clinically than many of the other words.
Because once the MRI suggests the nerve is actually being compressed or crowded, we begin paying much closer attention to whether the symptoms match that level and side.
Why MRI Findings Do Not Always Match The Pain
This is probably the single most important thing patients misunderstand.
An MRI can show lumbar disc disease very clearly.
That does not mean every visible finding is painful.
Systematic review evidence has long shown that the clinical importance of lumbar MRI findings remains uncertain in many situations, especially when trying to predict who will respond better to which treatment. Some trials suggest certain MRI findings may matter in specific contexts, but many findings are not straightforwardly actionable on their own.
And newer evidence still points in the same direction.
Disc degeneration can be associated with low back pain, but the relationship is not neat enough to say every MRI abnormality explains every symptom. Some studies suggest combined or summed MRI findings may relate more strongly to low-back-pain outcomes than single findings, which is another way of saying the picture is often more complex than one scary word on a report.
So yes, the MRI matters.
But symptoms still lead the conversation.
When MRI Matters More
There are times when the MRI becomes much more decisive.
For example:
- when the pain shoots clearly down the leg,
- when numbness or weakness follows a nerve-root pattern,
- when the imaging shows nerve root compromise that matches the symptoms,
- or when the question is whether surgery or another targeted treatment is solving a real structural problem.
That is where MRI becomes more than background description.
It becomes a map.
But even then, the map still has to match the patient standing in front of you.
Why One Scary MRI Word Should Not Decide The Whole Treatment Plan
This is where patients often go wrong on their own.
They read the worst-sounding phrase and build the entire story around it.
A report may contain six findings, but only one of them is truly relevant.
Or none of them fully explain the symptoms.
Or the biggest imaging abnormality may be old, while the current pain is coming from something more active but less dramatic.
That is why spine care is still interpretive.
Not automatic.
A report can describe.
It cannot decide.
What MRI Can Tell You Well
MRI is strong at showing:
- disc height loss,
- disc hydration changes,
- bulgings and herniations,
- annular fissures,
- spinal canal narrowing,
- foraminal narrowing,
- and possible nerve root compression.
That is valuable.
Because those findings help us understand structure.
And structure matters.
Especially when the patient has radicular pain, weakness, or a long course that is not improving.
What MRI Cannot Tell You By Itself
MRI cannot reliably answer all of these by itself:
- how much a patient hurts,
- how much fear is amplifying the pain,
- whether the visible change is old or active,
- whether the lower back pain is mostly discogenic, muscular, inflammatory, or mixed,
- or whether surgery will definitely help.
That is why careful examination, symptom pattern, timeline, and function still matter as much as the scan itself.
Why Some MRI Reports Sound Worse Than They Are
Radiology reports are written to describe everything visible.
That is their job.
They are not written to reassure patients.
So a report can sound heavy even when the actual clinical implication is modest.
This is not because the report is wrong.
It is because description and meaning are not the same thing.
That is why the same MRI sentence can create panic in a patient and a much more measured reaction in a spine specialist.
The doctor is not ignoring the finding.
They are ranking it.
When MRI Findings Should Worry Patients More
Usually not when the report simply says degeneration.
More concern is warranted when the MRI shows findings that clearly fit a more serious clinical picture, especially:
- large herniation with convincing nerve compression,
- marked canal or foraminal narrowing,
- nerve root compromise that matches progressive weakness,
- or findings that fit bladder, bowel, or saddle-area symptoms.
Those are the situations where MRI findings become more than background change.
They may start guiding urgent decisions.
FAQs About Lumbar Disc Disease On MRI

Does “degeneration” on MRI automatically mean something serious?
No. It means the disc shows signs of wear and structural change, but that does not automatically mean the finding is severe, dangerous, or the exact reason for the pain. MRI degeneration is common, and its meaning depends on symptoms and examination.
What is the difference between a bulging and a herniation on MRI?
A bulging is usually broader and less focal. A herniation is more specific and pushes disc material outward in a more defined way. The clinical importance depends less on the word alone and more on whether nearby nerves are being affected.
If my MRI looks bad, does that mean I need surgery?
Not automatically. MRI findings by themselves do not decide surgery. The key question is whether the scan matches the symptoms, the examination, and a clear structural target.
Can MRI explain my lower back pain completely?
Sometimes partly, but not always. MRI is excellent for structure, but structure alone does not fully explain pain. That is why clinical correlation still matters.
What MRI findings matter most for leg pain or sciatica?
Usually the ones suggesting nerve root irritation or compromise matter most, especially when the side and level match the symptoms.
Why did my report sound frightening even though my doctor was calm?
Because radiology reports describe abnormalities in technical language. They list what is visible, not how worried the patient should be. The doctor’s job is to decide which findings actually matter clinically.
Final Thoughts
Lumbar disc disease on MRI is important.
But it is not self-explanatory.
The scan can show structural truth very well.
It cannot tell the whole clinical story by itself.
That is why the best question after an MRI is rarely:
“How bad does this report sound?”
It is:
“Which of these findings actually explains what I am feeling?”
That is where a good interpretation begins.
And it is also where a lot of unnecessary fear ends.
When an MRI Check Makes Sense
MRI words can sound worse than they are. A report can show a lot, but it still does not always say why the back hurts.
So it helps to look at it with someone who reads these scans every day. What matters? What does not? Does it match the pain, the leg symptoms, or the weakness? That is usually where the report starts to make more sense.