Clinical Insights from Prof. Dr. Serdar Kabataş, MD, PhD (C)
First Signs That Something Has Changed in Crohn’s Biologic Therapy
Patients often remember the first months clearly. The pain became less. The bowel calmed down. Blood tests improved. Maybe the colonoscopy looked better. For the first time in a long while, the disease felt quieter.
Then, slowly, something changes.
A patient says: “The medicine worked at the beginning.”
Another says: “I was fine for two years, then the symptoms came back.”
Someone else says it more directly: “Doctor, I think my biologic stopped working.”
This is one of the most frustrating moments in Morbus Crohn treatment. Not because biologic therapy failed from the start. But because it gave hope first. It created stability. The patient trusted it. Then Crohn’s disease began to move again.
This does not always mean the medication is useless now. It also does not mean the patient did something wrong.
Crohn’s disease is a chronic immune-mediated disease. It can change over time. The immune system can find other inflammatory pathways. Drug levels can become too low. Antibodies may develop against a biologic. Sometimes symptoms return for a reason that is not active Crohn’s inflammation at all.
That is why we have to be careful.
When a patient has Crohn’s disease flare-ups while using biologic therapy, the first question should not be panic. The first question should be: What exactly has changed?
Table of Contents
Biologic Therapy for Crohn’s Disease Is Not One Single Treatment
Patients often use the word “biologic” as if it is one medicine.
It is not.
Biologic therapy for Crohn’s disease includes different drug groups. They target different parts of the immune response. Some block TNF-alpha. Some affect immune cell movement into the gut. Some target interleukin pathways involved in inflammation.
The names may be familiar to many patients:
- infliximab
- adalimumab
- vedolizumab
- ustekinumab
- risankizumab
- other advanced therapies depending on the country and case
Patients do not need to memorize all mechanisms. But they do need to understand one thing: Different biologics calm inflammation in different ways.
So if one biologic becomes weaker, it does not automatically mean all biologic therapy is finished. Sometimes the dose needs adjustment. Sometimes the interval needs review. Sometimes the drug level is low. Sometimes another pathway needs to be targeted.
And sometimes, yes, the disease has moved into a phase where medical therapy alone is not enough. That is the part patients fear.
But fear should not decide the next step. Assessment should.
Primary Non-Response and Loss of Response in Crohn’s Disease Are Not the Same Thing
There are two situations we separate in the clinic.
The first is primary non-response. This means the biologic never really worked. The patient started treatment, waited through the induction period, but symptoms, inflammation markers, imaging, or endoscopy did not improve enough.
The second is loss of response Crohn’s disease. This means the treatment worked first, then later became less effective.
Patients often mix these two together, but medically they are different. The reasons may be different. The next step may also be different.
A patient with primary non-response may have inflammation driven by a pathway that this biologic does not control well enough.
A patient with loss of response may have started well, then later developed low drug levels, antibodies, stronger inflammation, infection, fistula activity, or another complication.
So the sentence: “My biologic does not work” is not enough.
We need to know how it failed.
- Did it never work?
- Did it work and then fade?
- Did symptoms return but tests still look quiet?
- Did inflammation return on colonoscopy?
- Did a fistula become active again?
These are different problems.
Why Anti-TNF Failure Happens in Some Crohn’s Patients
Anti-TNF medicines changed Crohn’s disease treatment for many patients.
They can be very effective, especially in selected patients with active inflammation, fistulizing disease, or more aggressive disease patterns. But anti-TNF failure can happen.
Sometimes the body clears the medication too quickly. The drug level becomes too low before the next dose. The patient may feel better after treatment, then worse again before the next injection or infusion.
Sometimes the immune system develops antibodies against the drug. These antibodies can reduce the effect of the biologic or increase the risk of infusion or injection reactions.
Sometimes the inflammation is too strong for the current dose. Sometimes the disease mechanism is no longer mainly TNF-driven. And sometimes the problem is not the drug at all.
The patient may have:
- a narrowing in the intestine
- scar tissue
- a small abscess
- bile acid diarrhea after surgery
- irritable bowel symptoms on top of Crohn’s
- infection
- medication side effects
- stress on the body
- anemia
- nutritional weakness
This is why anti-TNF failure needs proper evaluation. Not guessing.
When Symptoms Return but the Disease Is Not Truly Active
This happens more often than patients expect. A patient has diarrhea, bloating, cramping, or urgency and thinks: “My Crohn’s is back.”
Sometimes it is. But sometimes the inflammation is not the main reason.
After years of Crohn’s disease, the bowel can become sensitive. Previous surgery can change digestion. Bile acids can irritate the colon. Small intestinal bacterial overgrowth may develop. Food intolerance may become more obvious. Stress and sleep problems may worsen gut symptoms. Some patients also have irritable bowel syndrome-like symptoms even when inflammation is controlled.
This does not mean the symptoms are imaginary. They are real. But the treatment is different.
If we assume every symptom is active Crohn’s inflammation, we may change a biologic too quickly. That can be a mistake.
Before changing strong medication, we need evidence. That may include:
- blood tests
- CRP and inflammation markers
- fecal calprotectin
- stool tests for infection
- drug level and antibody testing in selected cases
- MRI or CT enterography
- colonoscopy when needed
- pelvic MRI if perianal disease is present
The patient feels symptoms in the body. The doctor must find the cause behind them.
Drug Levels and Antibodies: Why Timing Matters
Biologic therapy is not only about the name of the medication. Timing matters. Dose matters. Interval matters. The body’s handling of the drug matters.
Some patients lose response because the level of biologic medicine in the blood becomes too low. This may happen because of body weight, inflammation burden, protein loss, fast clearance, missed doses, or individual metabolism.
In other patients, antibodies develop against the biologic. This can happen more often with some drugs than others. It may also be influenced by treatment interruptions, irregular dosing, or the absence of combination therapy in selected cases.
This is why doctors may check trough levels and anti-drug antibodies. A trough level means the amount of medication in the blood just before the next dose.
If the level is low and antibodies are absent, increasing the dose or shortening the interval may help some patients. If antibodies are high, changing treatment may be more logical. If the drug level is already good but inflammation is active, the disease may be escaping through a different pathway.
Then simply giving more of the same drug may not help.
This is where careful Crohn’s biologic therapy becomes very individual.
- One patient needs dose optimization.
- Another needs a switch within the same drug class.
- Another needs a different class.
- Another needs surgery.
- Another needs treatment of infection or abscess before anything else.
Same symptom. Different answer.
Crohn’s Disease Flare-Ups During Biologic Therapy
Crohn’s disease flare-ups during biologic therapy can feel very discouraging.
Patients often say: “But I am already on the strong medicine.”
That is true. But strong medicine does not make Crohn’s disease disappear as a possibility.
A flare can happen because the drug effect is no longer enough. It can also happen after infection, antibiotics, stress on the body, smoking, missed doses, stopping another medication, or disease progression.
Sometimes the flare is mild. Sometimes it is a warning.
Patients should be especially careful with symptoms like fever, severe abdominal pain, vomiting, rapidly worsening weakness, dehydration, heavy bleeding, or painful swelling near the anus.
These are not symptoms to watch quietly for weeks.
A Crohn’s flare under biologic therapy should be assessed early, because waiting can allow inflammation to become more complicated.
Crohn’s disease can create:
- ulcers
- narrowing
- fistulas
- abscesses
The goal is not only to make symptoms quieter. The goal is to prevent damage.
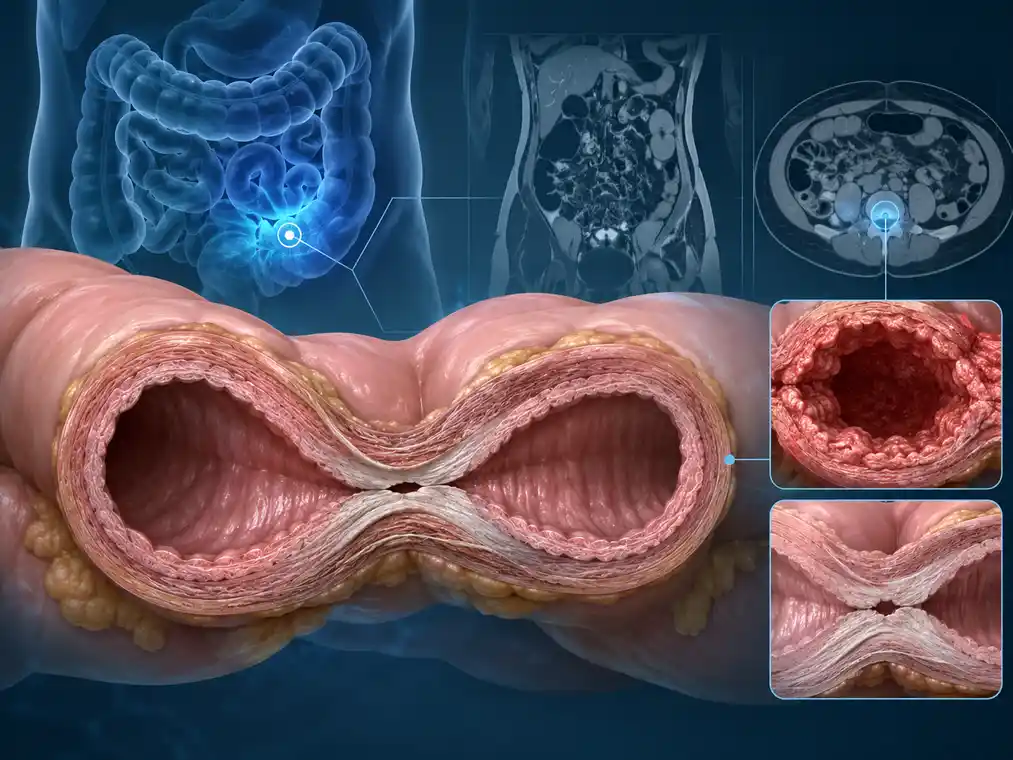
When the Problem Is Scar Tissue, Not Active Inflammation
This is a very important point.
Biologic therapy treats inflammation. It does not melt scar tissue.
In Crohn’s disease, long-term inflammation can sometimes lead to strictures. A stricture is a narrowed area of bowel. Some strictures are mainly inflammatory and may improve with medical treatment. Others are mainly fibrotic, meaning scar-related.
Patients with strictures may say:
- “I feel blocked.”
- “I cannot eat normally.”
- “I get cramps after meals.”
- “My stomach swells.”
- “I vomit when it gets bad.”
If a patient has scar-related narrowing, increasing biologic therapy may not solve the mechanical problem.
This is where imaging matters.
Sometimes we need MRI enterography, CT enterography, intestinal ultrasound, endoscopy, or surgical evaluation. Not because we are rushing to surgery. But because we need to understand the structure of the bowel.
If the road is inflamed, medicine may calm it. If the road is narrowed by scar, medicine has limits.
This is one reason biologic therapy can appear to “stop working,” when actually the disease has changed its shape.
Perianal Disease Can Break the Pattern
Some Crohn’s patients have bowel symptoms under control, but perianal disease remains active.
This is confusing for patients.
They may say: “My stomach is better, but the fistula is not.”
Or: “My blood tests are fine, but I still have drainage.”
Perianal Crohn’s disease does not always behave exactly like intestinal Crohn’s disease. Fistulas may need drainage, seton placement, pelvic MRI, antibiotic support in selected situations, biologic optimization, and colorectal surgical care.
A biologic may help, but it may not be enough alone.
If there is an abscess, it must be treated. If the fistula anatomy is complex, it must be mapped. If the rectum is inflamed, that changes the plan.
This is why a patient with drainage should not only ask: “Is my biologic failing?”
Sometimes the better question is: “What is the fistula doing anatomically?”
That is a different kind of question. And it needs a different kind of evaluation.
Why Doctors Sometimes Change Biologic Therapy
Changing biologic therapy is not a small decision.
Patients worry about it.
They ask:
- “What if the next one also fails?”
- “What if I run out of options?”
- “What if I should have changed earlier?”
These are normal fears.
A doctor may consider changing biologic therapy when there is clear evidence of active disease despite proper dosing, when antibodies reduce the drug effect, when side effects become unacceptable, or when the disease pattern suggests another mechanism should be targeted.
But the decision should not be emotional only.
It should be based on the full picture:
- symptoms
- blood tests
- stool inflammation markers
- endoscopy
- imaging
- drug level and antibody results when useful
- fistula status if present
- previous treatment history
- infection risk
- surgical history
- patient preference
This is the reason Crohn’s treatment can feel slow from the outside. The doctor is not only choosing the next drug. The doctor is trying to avoid the wrong next drug.
What Patients Should Not Do Alone
A patient who feels that biologic therapy is no longer working may become frustrated. That is understandable.
But some decisions should not be made alone.
- Do not stop biologic therapy suddenly without medical advice.
- Do not delay care during severe symptoms.
- Do not restart old steroids without a plan.
- Do not assume every flare means the biologic has failed.
- Do not assume every symptom is Crohn’s inflammation.
- Do not ignore fever, abscess-like swelling, vomiting, severe pain, or dehydration.
Stopping and starting biologics irregularly can sometimes make future treatment more difficult. It may increase the risk of antibodies with some medications. It can also allow inflammation to return in a more aggressive way.
Crohn’s disease does not like gaps in thinking. Treatment changes should be planned.
Where Advanced Treatment Discussions May Begin
When a patient has tried several biologics, had dose optimization, still has active inflammation, or develops complications, the conversation naturally becomes wider.
This does not mean abandoning standard medicine. It means asking carefully:
- What is still active?
- What is damaged?
- What is inflammatory?
- What is scar-related?
- What is surgical?
- What is immune-driven?
- What is realistic to improve?
This is also the point where some patients begin asking about regenerative medicine, stem cells, or other supportive approaches. That question should not be dismissed automatically. But it also should not replace the basic Crohn’s assessment.
In selected patients, especially those with difficult fistulizing disease or complex inflammatory patterns, regenerative medicine may be discussed carefully as a supportive field. It is not a cure. It is not a replacement for biologic therapy. It is not a way to avoid urgent surgery when surgery is needed.
The wider discussion only becomes useful when the disease picture is clear.
This is why, in the broader Morbus Crohn treatment pathway, stem cell therapy for Morbus Crohn should be considered only after proper evaluation and realistic medical framing.
Safety Signs During Biologic Therapy
Biologic medicines affect the immune system. For many patients, they are used safely and effectively. But infections and complications must be taken seriously.
Patients using biologic therapy should seek urgent medical care if they develop high fever, severe abdominal pain, persistent vomiting, shortness of breath, chest pain, confusion, severe weakness, dehydration, black stool, heavy rectal bleeding, or painful swelling near the anus.
A painful lump near the anus with fever may be an abscess. Severe abdominal pain with vomiting may suggest obstruction. Fever during immune-suppressive treatment should not be ignored.
This is not written to frighten patients. It is written because timing matters.
In Crohn’s disease, late treatment of complications can make the next step harder.
How I Usually Explain Crohn’s Biologic Therapy in the Clinic
When a patient says, “My biologic stopped working,” I try not to answer too quickly.
First, I ask when it worked. Then when it changed. Then what changed.
- Was it pain?
- Diarrhea?
- Bleeding?
- Weight loss?
- Fatigue?
- Fistula drainage?
- Fever?
- Blood tests?
- Colonoscopy?
- MRI?
The treatment decision depends on the answer.
Sometimes the biologic is still useful, but the dose needs adjustment. Sometimes antibodies have appeared. Sometimes the disease needs a different mechanism. Sometimes the bowel has developed scar-related narrowing. Sometimes there is infection or abscess. Sometimes the patient’s symptoms are real, but not driven by active Crohn’s inflammation.
This is why the phrase “not working” is only the beginning of the conversation.
Not the end.
Final Thoughts on Crohn’s Biologic Therapy
Biologic therapy for Crohn’s disease can change a patient’s life. But it is not always a straight road.
Some patients respond well and stay stable for years. Some never respond enough. Some improve first, then slowly lose response. Some appear to fail biologic therapy, but the real issue is scar tissue, infection, fistula anatomy, or another cause of symptoms.
That is why the next step should not be chosen only by fear. It should be chosen by understanding.
When Crohn’s biologic therapy becomes weaker, the question is not only: “What medicine comes next?”
The better question is: “Why is the disease active again?”
That is where good treatment decisions begin.
Frequently Asked Questions About Crohn’s Biologic Therapy

Why did my biologic work first and then stop helping?
There are several possible reasons.
The drug level may be too low. Antibodies may have developed. The inflammation may now be driven by another pathway. Or the symptoms may be coming from scar tissue, infection, fistula activity, or another bowel problem.
We should not guess too quickly. The reason matters because the next step changes.
Does a flare mean my biologic therapy for Crohn’s disease has failed?
Not always.
A flare during biologic therapy needs evaluation. Sometimes it means the medicine is not enough anymore. Sometimes the dose or interval needs adjustment. Sometimes there is infection or another cause of symptoms.
One bad week does not always mean the treatment is finished. But repeated symptoms should be checked.
What is anti-TNF failure?
Anti-TNF failure means that medicines targeting TNF-alpha are not controlling the Crohn’s disease well enough.
This may happen from the beginning, or after a period of good response. If it happens later, we often look at drug levels, antibodies, inflammation markers, imaging, and the full disease pattern before deciding what to do next.
Can I switch to another biologic?
Sometimes, yes.
But the choice depends on why the first biologic is not working. If the drug level is low, dose optimization may be considered. If antibodies are high, switching may be more logical. If the disease is active despite a good drug level, another drug class may be needed.
This decision should be individual.
Should I stop my biologic if I feel it is not working?
No, not without medical advice.
Stopping suddenly can allow inflammation to return or worsen. In some cases, irregular treatment may also make future use more difficult. If you feel the biologic is no longer helping, the safer step is to investigate why.