Clinical Insights from Prof. Dr. Serdar Kabataş, MD, PhD (C)
Stem Cell Therapy for Morbus Crohn: Why the Conversation Must Start Carefully
Patients with Morbus Crohn usually do not ask about stem cells at the beginning of the disease.
They ask after years. After medications. After flare-ups. After colonoscopy reports they no longer want to read.
Sometimes after surgery. Sometimes after a fistula that does not close.
A patient may say:
“I am tired of inflammation.”
Another says:
“My body calms down, then it starts again.”
Someone else comes with a quieter sentence:
“Doctor, I just want a normal day.”
This is where the discussion about stem cell therapy for Morbus Crohn often begins. Not from curiosity. From fatigue.
And that matters.
Because regenerative medicine should never be presented as a shortcut around proper Crohn’s disease care. Morbus Crohn is a chronic inflammatory bowel disease. It can affect different parts of the digestive tract. It can behave mildly in one patient and aggressively in another.
The same diagnosis does not mean the same disease story.
Before we speak about stem cells, exosomes, or any supportive regenerative approach, we first need to understand the patient’s Crohn’s pattern.
- Where is the inflammation?
- How active is it?
- Is there narrowing?
- Is there abscess?
- Is there fistula?
- Has surgery already been done?
- Are biologic medicines working, partly working, or no longer working?
These questions are not small details. This is why stem cell therapy for Morbus Crohn should never be discussed before the disease pattern is clear.
They decide whether regenerative medicine is even a reasonable discussion.
Table of Contents
What Morbus Crohn Usually Means in Real Life
Morbus Crohn is not only diarrhea.
Many patients already know this.
It may come with abdominal pain, urgency, weight loss, fatigue, fever, anemia, poor appetite, mouth ulcers, joint pain, skin problems, or repeated infections around the anus.
But symptoms do not always tell the full truth.
Some patients have strong symptoms with moderate inflammation. Some have dangerous inflammation and surprisingly little pain. Some look well from the outside but live around toilets, diet restrictions, and fear of the next flare.
A Crohn’s patient may say:
“I do not trust my stomach anymore.”
That sentence is not medical terminology. But clinically, it tells us a lot.
Crohn’s disease changes how a person plans the day. Travel. Food. Work. Sleep. Social life. Even confidence.
This is why treatment cannot only focus on one laboratory value.
We need to understand the disease and the person carrying it.
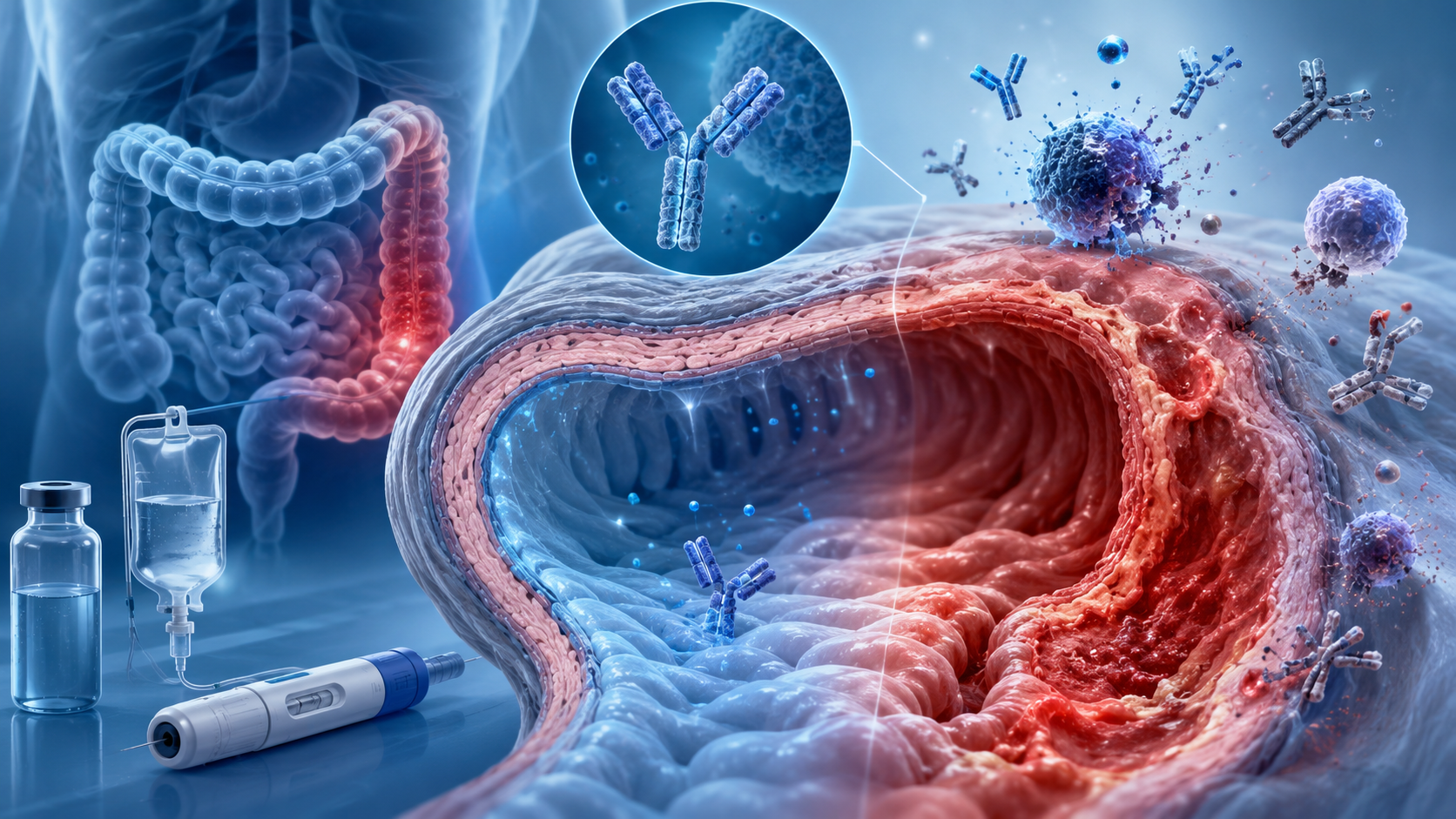
Why Crohn’s Disease Inflammation Becomes So Difficult to Control
Crohn’s disease is an immune-mediated condition.
The immune system reacts in a way that keeps inflammation active in the gut wall. The lining of the intestine becomes irritated. The deeper layers may become involved. Over time, inflammation may cause ulcers, thickening, narrowing, scar tissue, fistulas, or abscess formation.
This is one reason Crohn’s is different from a simple stomach infection.
An infection usually comes and goes.
Crohn’s may calm down, then return. It may move in waves.
Some patients have long quiet periods. Some have repeated flares. Some have inflammation that does not fully switch off even with strong treatment.
The mechanism is not one single switch. It includes immune cells, inflammatory signals, gut barrier function, microbiome changes, genetics, environmental triggers, nutrition, stress on the body, previous infections, and sometimes smoking.
Medicine is rarely neat.
That is why two patients with Morbus Crohn may need very different treatment plans.
One patient may do well with standard medication. Another may need biologic therapy. Another may need surgery. Another may have a perianal fistula that becomes the main problem, even when intestinal symptoms are not dramatic.
This is also where stem cell therapy enters the conversation.
But only carefully.
Standard Morbus Crohn Treatment Remains the Foundation
This part should be very clear.
Stem cell therapy for Morbus Crohn is not the foundation of treatment.
The foundation is still proper gastroenterology care.
Stem cell therapy for Morbus Crohn, if considered, belongs after that basic medical work is done.
That may include anti-inflammatory treatment, immune-modifying medication, biologic medicines, small molecule therapies, antibiotics in selected situations, nutritional support, iron or vitamin correction, endoscopic monitoring, imaging, and surgery when needed.
For some patients, biologic medicines such as anti-TNF agents, anti-integrin therapy, anti-interleukin therapy, or other advanced treatments can change the course of the disease.
For some patients, surgery is not a failure.
It is the correct treatment at the correct time.
Patients sometimes see surgery as “the last thing.”
But in Crohn’s disease, waiting too long with an abscess, severe narrowing, or uncontrolled fistula may create more damage.
So the question is not:
“How can we avoid all standard treatment?”
The better question is:
“What is the safest and most logical sequence for this patient?”
Regenerative medicine, if considered, should be placed inside that sequence. Not above it. Not instead of it.
Where Crohn’s Disease Stem Cell Therapy May Fit
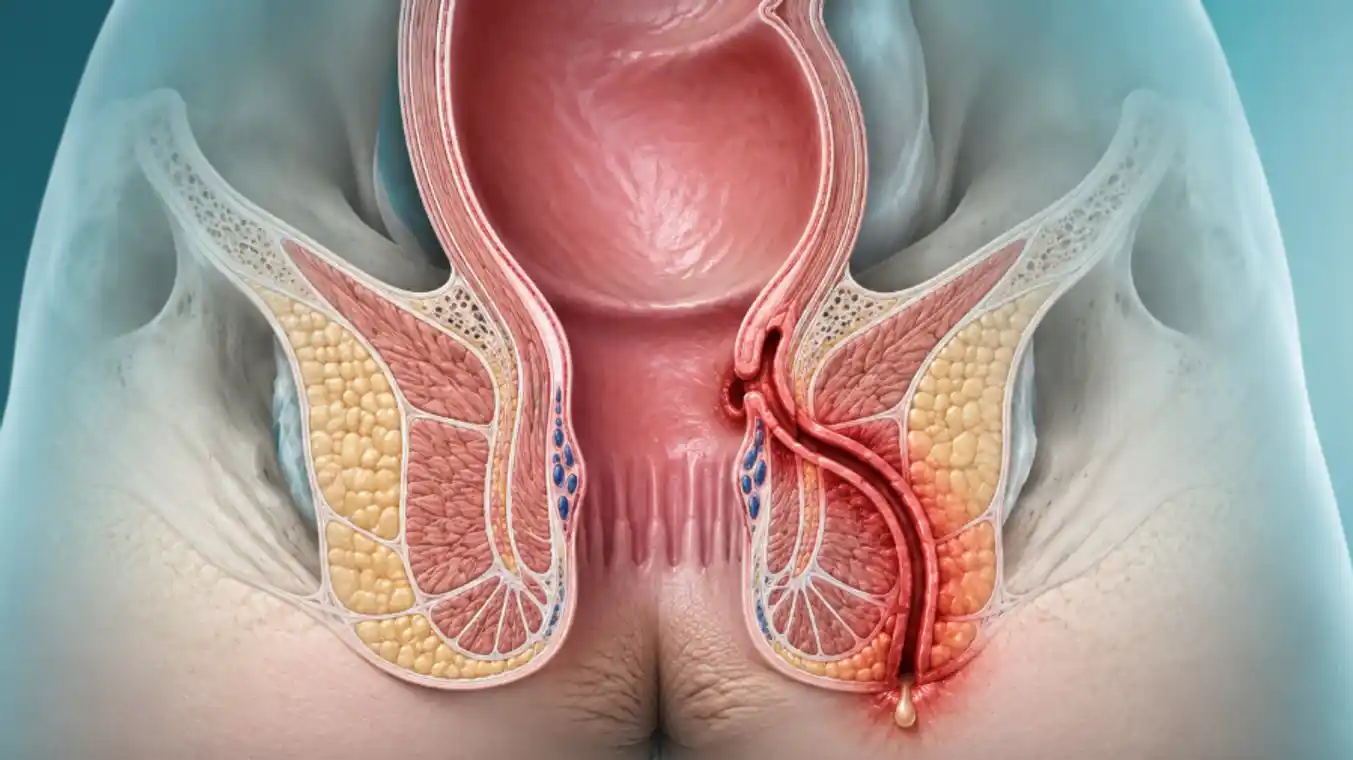
The most serious discussion around stem cells in Crohn’s disease has been in patients with difficult perianal fistulas.
This means abnormal tunnels near the anus or rectum, often linked to chronic inflammation. These fistulas may drain fluid, cause pain, form abscesses, and return even after treatment.
Patients describe it in very simple words:
- “It closes, then opens again.”
- “I cannot sit comfortably.”
- “I am afraid of another abscess.”
This group of patients can be very difficult to treat.
Standard care may include antibiotics, drainage of abscesses, seton placement, biologic therapy, surgical care, and long-term follow-up. In selected cases, mesenchymal stem cells have been studied as a local supportive treatment for complex perianal fistulas.
The idea is not that stem cells “become a new intestine.”
The more realistic idea is that mesenchymal stem cells may influence inflammation, immune signaling, tissue repair signals, and the local wound environment.
In other words, they may help create a better environment for healing in selected fistula cases.
May. Not always. Not for everyone.
And not without proper preparation.
If there is an abscess, it must be treated. If there is uncontrolled active Crohn’s inflammation, that must be addressed. If the anatomy of the fistula is complex, imaging and surgical evaluation matter.
A stem cell discussion without fistula mapping is not serious medicine.
This is one reason stem cell therapy for Morbus Crohn is usually discussed most carefully in selected fistula cases.
Stem Cells for Intestinal Crohn’s Disease: A More Cautious Area
Many patients ask a broader question:
“Can stem cells heal my Crohn’s disease inside the intestine?”
This is where we must slow down.
For intestinal, or luminal, Crohn’s disease, stem cell therapy remains much less established than patients often imagine. Research exists. Interest exists. Some early studies and reviews discuss possible immune-modulating effects.
But this does not mean stem cells are a proven routine treatment for intestinal Crohn’s disease.
Crohn’s inflammation inside the bowel is complex. A patient may have ulcers, narrowing, scar tissue, active inflammation, bacterial complications, nutritional weakness, or previous surgery. These are not all the same problem.
Stem cells cannot be discussed as one answer for all of them.
If the intestine is narrowed mainly by scar tissue, calming inflammation may not open the scar. If there is an abscess, regenerative medicine is not the priority. If there is severe malnutrition, that must be corrected. If biologic treatment has not been optimized, that discussion comes first.
This is why careful evaluation is not a formality.
It is the treatment.
How Stem Cells May Work in Morbus Crohn: The Medical Mechanism
Patients often think stem cells repair the body by turning into new tissue.
That is only a small and often misleading part of the story.
In Crohn’s disease, the more relevant discussion is immunomodulation.
Mesenchymal stem cells may release signals that interact with immune cells. They may influence inflammatory pathways. They may affect macrophages, T cells, cytokines, and tissue repair responses. They may help reduce an overly aggressive local immune reaction in certain environments.
This is the reason researchers have studied them in inflammatory diseases.
But biology is not the same as guaranteed clinical success.
A cell can show interesting behavior in the laboratory. A small trial can show promise. A patient group can respond partly. Then a larger study may show less benefit than expected.
That is medicine.
Especially in Crohn’s disease.
The immune system is not simple. The bowel is not simple. Fistulas are not simple.
So when we explain stem cell therapy for Morbus Crohn, the honest explanation is this:
Stem cells are being studied because they may help regulate inflammation and support tissue healing signals.
They are not proven to cure Crohn’s disease.
They are not a replacement for biologics, surgery, drainage, colonoscopy follow-up, or standard inflammatory bowel disease care.
That sentence may sound less exciting.
But it is safer.
And usually more truthful.
Exosome Therapy for Crohn’s Disease: What We Can and Cannot Say
Exosomes are now mentioned everywhere.
Sometimes too quickly.
Stem cells and exosomes are related, but they are not the same thing.
Stem cells are living cells.
Exosomes are tiny signal-carrying particles released by cells. They carry proteins, lipids, RNA fragments, and other biological messages. They do not divide. They do not become bowel tissue. They do not “turn into” intestine.
They are messengers.
This is why exosomes are interesting in inflammatory diseases like Crohn’s disease. The question is whether these signals can help influence immune behavior, inflammation, tissue repair, and the gut environment.
It is a reasonable research question.
But it is still a research question.
For Morbus Crohn, exosome therapy should not be described as a proven cure. It should not be sold as a guaranteed way to stop flare-ups. It should not replace medication that is controlling the disease.
At this stage, exosomes belong in a careful investigational discussion.
Maybe one day, exosome-based treatments will become more standardized. Maybe they will help selected patients. Maybe research will show which type, dose, source, and timing are useful.
But today, we still need more clinical data. We need consistency. We need safety monitoring. We need proper patient selection.
The principle is the same like in other chronic inflammatory fields, including respiratory diseases such as COPD.
Interesting biology is not enough.
The patient needs honest medicine.
What Regenerative Medicine Cannot Promise in Crohn’s Disease
This section is necessary.
Because patients with Crohn’s disease are often tired.
And tired patients can become vulnerable to strong promises.
Regenerative medicine cannot promise to cure Morbus Crohn.
- It cannot promise that biologic medicines will no longer be needed.
- It cannot promise that surgery will be avoided.
- It cannot promise that fistulas will close permanently.
- It cannot promise that scar tissue will disappear.
- It cannot promise that flare-ups will never return.
- It cannot promise that the immune system will “reset” in a predictable way.
This does not mean the field has no value.
It means we must speak accurately.
For selected patients, especially those with difficult perianal fistulizing Crohn’s disease, regenerative approaches may be discussed as part of a broader treatment plan. In other patients, the answer may be no. Or not now. Or only inside a research-based setting.
A careful no is sometimes better medicine than an easy yes.
Perianal Fistula in Crohn’s Disease: Why This Patient Needs Special Attention
This patient needs special attention.
Perianal Crohn’s disease can be one of the most frustrating forms of Morbus Crohn.
The bowel symptoms may be quiet, but the fistula continues. Or the patient may have both active bowel disease and fistula drainage.
Sometimes there is pain. Sometimes fever. Sometimes swelling. Sometimes repeated abscesses.
Patients may feel embarrassed to speak about it. They may delay the visit. They may try to manage drainage quietly for months.
They should not feel ashamed.
Perianal Crohn’s disease is a medical problem, not a personal failure.
Before any regenerative treatment is discussed, the basics must be clear.
- Is there an abscess?
- How many fistula tracts are present?
- Is the rectum inflamed?
- Has MRI been done?
- Is there a seton?
- Is biologic therapy optimized?
- Is surgery needed first?
In this area, coordination matters. Gastroenterology and colorectal surgery often need to work together. Stem cell therapy, if considered, usually belongs after proper drainage, infection control, imaging, and disease assessment.
Not before.
When Stem Cell Therapy Should Not Be the First Question
Sometimes patients arrive asking only one thing:
“Can I have stem cells?”
But the medical question may be different.
- If there is severe active inflammation, we need to control inflammation.
- If there is a bowel obstruction, we need to understand whether it is inflammation or scar.
- If there is an abscess, it needs urgent treatment.
- If there is fever and severe pain, waiting is unsafe.
- If the patient is losing weight quickly, nutrition and disease activity need attention.
- If blood tests show serious anemia or infection, this changes the plan.
Stem cells are not emergency treatment.
Exosomes are not emergency treatment.
Regenerative medicine is not the answer to every difficult Crohn’s moment.
Sometimes the correct treatment is antibiotics. Sometimes drainage. Sometimes steroids for a short period. Sometimes biologic change. Sometimes surgery. Sometimes nutritional rebuilding. Sometimes simply re-checking the diagnosis and disease location.
Crohn’s disease punishes shortcuts.
Safety Signs Patients Should Not Ignore
Some symptoms should not be watched at home for too long.
Severe abdominal pain, persistent vomiting, a swollen abdomen, high fever, chills, fainting, heavy rectal bleeding, black stool, severe dehydration, confusion, or rapidly worsening weakness need urgent medical attention.
A painful swelling near the anus with fever may mean abscess.
That should not wait for a regenerative medicine appointment.
Severe abdominal pain with vomiting may mean obstruction.
That also should not wait.
Crohn’s patients often become strong because they live with symptoms for years.
But strength can sometimes make patients wait too long.
There are moments when waiting is not bravery.
It is risk.
How I Usually Explain Stem Cell Therapy for Morbus Crohn in the Clinic
I usually try to separate hope from pressure.
Hope is allowed.
Pressure is not.
A patient with Morbus Crohn has the right to ask about new treatments. They have the right to ask about stem cells. They have the right to ask about exosomes.
But they also have the right to receive a careful answer.
I usually explain it like this:
First, we understand your Crohn’s disease today.
Not five years ago.
Today.
Then we ask what the main problem is.
- Active bowel inflammation?
- Perianal fistula?
- Scar-related narrowing?
- Repeated abscess?
- Medication failure?
- Poor healing?
- Fatigue and nutritional weakness?
Each one has a different answer.
If regenerative medicine has a place, it should fit the problem clearly. If it does not fit, we should not force it.
Advanced medicine is not using the newest word. Advanced medicine is choosing the right treatment for the right patient at the right time.
Final Thoughts on Stem Cell Therapy for Morbus Crohn
Stem cell therapy for Morbus Crohn is not a simple yes or no subject.
It is a careful subject.
The value of stem cell therapy for Morbus Crohn depends on the disease pattern, the complications, and the timing.
There is real scientific interest, especially around mesenchymal stem cells and difficult perianal fistulas. There is also growing curiosity around exosomes and immune signaling.
But Crohn’s disease is not one disease pattern.
And regenerative medicine is not a cure.
For some patients, it may become part of a supportive discussion after proper evaluation. For others, the safest answer may be to optimize standard Crohn’s care first.
The better question is not only:
“Can stem cells help Crohn’s disease?”
The better question is:
“What exactly is my Crohn’s disease doing right now?”
That is where honest treatment begins.
Frequently Asked Questions About Stem Cell Therapy for Morbus Crohn

Can stem cell therapy cure Morbus Crohn?
No.
I would not use the word cure.
Crohn’s disease is chronic and immune-mediated. Stem cells are being studied because they may influence inflammation and healing signals, especially in selected fistula cases. But they do not erase the disease. They do not replace proper Crohn’s treatment.
Is stem cell therapy useful for every Crohn’s patient?
No.
The patient with a perianal fistula is very different from the patient with small bowel narrowing. And both are different from a patient with mild inflammation controlled by medication.
This is why we first need to know the disease pattern. Without that, “stem cell therapy” is just a general phrase.
What if I have a Crohn’s fistula that keeps coming back?
Then the fistula needs proper evaluation.
Usually we need imaging, often pelvic MRI, and a careful look at whether there is abscess, active rectal inflammation, seton placement, and whether biologic treatment is optimized.
In selected complex perianal fistulas, stem cell-based treatment has been studied. But it should not be discussed alone, without the surgical and gastroenterology plan.
Are exosomes better than stem cells for Crohn’s disease?
We cannot honestly say that.
Exosomes are interesting because they carry cell signals and may affect inflammation. But for Crohn’s disease, this is still investigational. The science is moving, but it is not settled.
I would be careful with anyone who gives a very confident answer here.
Should I stop my Crohn’s medication if I am considering regenerative medicine?
That would be unsafe for many patients.
If regenerative medicine is considered, it should be discussed around the existing Crohn’s treatment plan, not as a sudden replacement. Stopping medication can trigger a flare, and in Crohn’s disease a flare is not always easy to control again.
When a Careful Review Makes Sense
Morbus Crohn does not behave the same way in every patient. Some patients struggle mainly with inflammation. Some with fistulas. Some with medication failure, scar-related narrowing, or repeated flare-ups.
If you are wondering whether regenerative medicine may have a supportive role in your case, the first step is not a promise. It is a careful review of your diagnosis, reports, previous treatments, and current disease pattern.