Regenerative Medicine

Clinical Insights from Prof. Dr. Serdar Kabataş, MD, PhD (C)
When patients ask me about asthma vs COPD, it is usually not because they want a textbook definition. They come because something does not feel right anymore: more cough, more wheezing, more pauses while walking, more dependence on inhalers — and sometimes two different diagnoses written in two different reports.
Breathing diseases are sometimes given simple names.
But patients rarely arrive as simple textbook cases.
One patient says, “I had asthma when I was young, but now they tell me it is COPD.”
Another says, “My inhaler helps, but not enough.”
Someone else brings old reports, new reports, different diagnoses, and the same tired sentence:
“I just want to understand what is happening to my lungs.”
This is a very reasonable wish.
Asthma and COPD can look similar. Both may cause wheezing. Both may cause cough. Both may create pressure in the chest. Both can make stairs feel longer than they really are.
But they are not the same disease.
And before we speak about regenerative medicine, stem cells, exosomes, or any advanced supportive treatment, we have to start there.
Not with the treatment.
With the diagnosis.
Because if we do not understand the lung problem correctly, even the most advanced treatment discussion becomes weak.
The confusion usually begins with symptoms.
From the outside, asthma and COPD may look almost identical.
But inside the body, the story is often different.
Asthma usually behaves like a condition that changes. It may be quiet for days or weeks, then suddenly become active. A patient may be fine in the morning and worse at night. Fine at home, worse outside. Fine in summer, worse in spring. Fine until dust, pollen, cold air, exercise, smoke, perfume, infection or stress triggers the airways.
COPD is often less dramatic at the beginning.
It creeps in.
Many patients do not remember the first day they became breathless. They only remember the adjustments.
Nobody calls these things “disease progression” at first.
They feel like age. Or tiredness. Or being out of shape.
But sometimes, this is how COPD enters a person’s life. Quietly. Without asking permission.
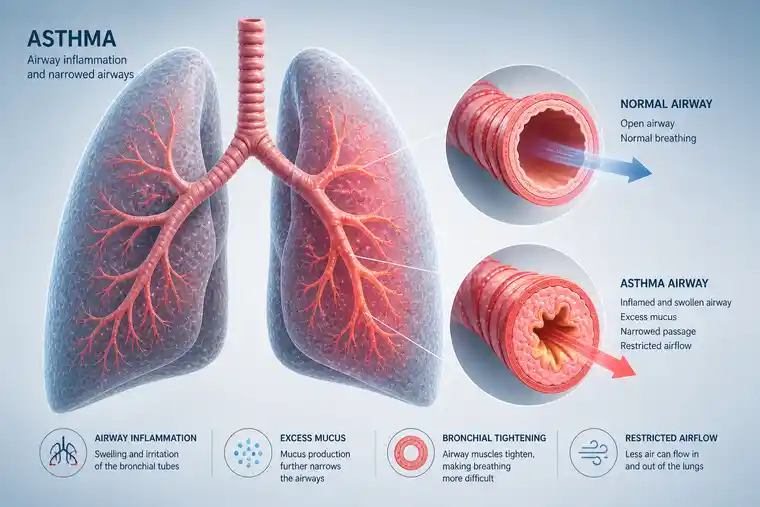
Asthma is mainly a disease of sensitive, reactive airways.
The airways become inflamed. The muscles around them tighten. Mucus may increase. Air has difficulty moving in and out. The patient may cough, wheeze, feel chest tightness or become short of breath.
But the important point is this:
Asthma often changes.
It has moods, almost.
Some days are good. Some nights are bad. A patient may feel normal between attacks. Another patient may have daily symptoms, but still notice clear triggers. Cold air. Dust. Cats. Mold. Exercise. Viral infections. Strong smells. Seasonal allergy.
Many asthma patients also have a history that gives us clues. Childhood wheezing. Allergies. Eczema. Family history. Symptoms that began early in life. Symptoms that improve strongly with the right inhaled treatment.
Of course, asthma can also begin in adulthood. And not every asthma patient has allergies.
Medicine is never that neat.
But in general, asthma is more reversible than COPD. The airways can often open significantly with proper treatment. Inflammation can often be controlled. Attacks can often be reduced.
That is why asthma deserves proper treatment, not assumptions.
A person who has uncontrolled asthma should not immediately be told, “This is COPD now.”
Sometimes it is still asthma.
Just not well controlled.
COPD means Chronic Obstructive Pulmonary Disease.
In Turkish, most patients know it as KOAH.
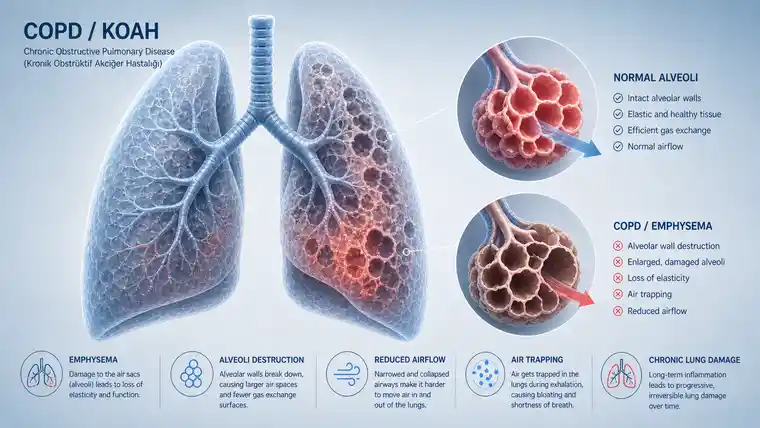
COPD is different from asthma because the breathing limitation is usually more persistent. The airways are not only sensitive; they are often structurally changed. The small airways may become narrowed. The lung tissue may lose elasticity. Air may become trapped. In emphysema, the tiny air sacs are damaged. In chronic bronchitis, mucus and cough become part of daily life.
The patient may say:
These sentences are important.
COPD is often linked to smoking, but it is not only a smoker’s disease. Long-term exposure to polluted air, occupational dust, chemical fumes, repeated infections and poorly controlled airway inflammation may all play a role. Some people are more vulnerable than others.
And COPD does not move at the same speed in every patient.
That last part matters.
Because COPD is not only a disease of the lungs. It also changes how a person moves through the world.
A patient begins to calculate distance.
They look for chairs.
They avoid long conversations.
They worry about the next infection.
This is the part that spirometry does not fully show.
Asthma is usually more variable.
COPD is usually more persistent.
That is not a perfect rule. There are exceptions. But it helps patients understand the pattern.
Asthma often comes with attacks, triggers and better periods. COPD often creates a baseline limitation that slowly becomes part of the patient’s daily life.
Another difference is reversibility.
In asthma, airway narrowing often improves clearly after bronchodilator medication or anti-inflammatory treatment. In COPD, the airways may improve partly, but the obstruction usually does not disappear completely.
This is why pulmonary function testing is so important.
We should not diagnose only by listening to symptoms. We need spirometry. We need to see how much air the patient can blow out, how fast, and how much changes after medication. Sometimes we need imaging. Sometimes blood tests. Sometimes oxygen assessment. Sometimes we need to look again at a diagnosis that was made years ago and never questioned.
Patients often say, “But doctor, I already know my diagnosis.”
Maybe.
But sometimes old labels stay in the file longer than they should.
Some patients do not fit cleanly into one box.
They may have asthma features and COPD features together.
For example, a patient may have had asthma since youth, but later developed fixed airway obstruction after years of smoking or pollution exposure. Another patient may have COPD but also strong allergic symptoms, eosinophilic inflammation or wheezing that varies more than expected.
These are the patients who create real clinical thinking.
They may say:
In these cases, the question is not always, “Is it asthma or COPD?”
Sometimes the better question is:
How much of this disease behaves like asthma, and how much behaves like COPD?
That answer matters because treatment changes.
Asthma-like inflammation may need one approach. COPD-type obstruction and flare-up risk may need another. The patient’s age, history, exposures, lung function, imaging and response to treatment all matter.
This is also where mistakes can happen.
If asthma features are missed, the patient may not receive enough anti-inflammatory airway treatment.
If COPD features are missed, the patient may not receive proper COPD management, pulmonary rehabilitation, vaccination planning or flare-up prevention.
A name on paper is not enough.
The pattern must be understood.
Many patients ask about regenerative medicine when they feel standard treatment is not giving them enough.
I understand this.
When breathing becomes limited, people search. They read. They ask friends. They watch videos. They compare treatments. They want something that does not only open the airway for a few hours, but maybe calms the deeper process.
That wish is human.
But regenerative medicine should not be used to escape diagnosis.
It should come after diagnosis.
Before discussing stem cells or exosomes, we need to know several things:

In COPD, regenerative medicine is discussed mainly because inflammation does not fully switch off.
The lung remains irritated. The immune system may continue sending signals. The airways stay vulnerable. Infections or flare-ups can push the lungs into another period of injury, then recovery, then sometimes incomplete recovery.
Stem cells and exosomes are being studied because they may influence this inflammatory environment.
Regenerative medicine does not grow new lungs.
It does not rebuild destroyed alveoli in a predictable way.
It does not erase emphysema.
It does not replace inhalers or oxygen.
The possible role is more modest, but still meaningful for selected patients.
The aim is to support immune balance, calm excessive inflammatory signaling, improve the tissue environment, and possibly help some patients experience fewer flare-ups, better tolerance for daily activity or a more stable course.
Sometimes patients expect dramatic words.
But in COPD, small changes may matter.
Being able to walk a little further.
Recovering better after exertion.
Having fewer bad weeks.
Sleeping with less effort.
Needing fewer pauses.
These are not miracle claims. They are the kind of changes patients often care about most.
But they are not guaranteed.
And they must be discussed honestly.
Exosomes are often mentioned together with stem cells, but they are not the same thing.
Stem cells are living cells.
Exosomes are tiny signal-carrying particles released by cells. They do not divide. They do not become lung tissue. They act more like messengers.
That is why exosomes are interesting in chronic inflammatory diseases. The question is whether these signals can help influence immune behavior and inflammatory activity in a useful way.
In COPD, this idea is biologically interesting because inflammation plays such a large role. But biologically interesting does not mean fully proven.
Patients should understand that difference.
There is research. There is clinical interest. There are patients who may report meaningful improvement. But there are also limits. COPD is complex. Lung damage is not all the same. A patient with mild chronic bronchitis is not the same as a patient with severe emphysema and low oxygen.
So the discussion must stay personal.
Not “Does it work for COPD?” as a general slogan.
But:
Could this have a reasonable supportive role for this patient, at this stage, with this lung condition?
That is the better question.

No. This is where we must be careful.
Asthma has strong established treatments. Many patients improve very well with correct inhaled therapy, trigger control and regular follow-up. In more severe asthma, modern biologic medications may target specific inflammatory pathways.
So regenerative medicine should not be presented as a standard asthma treatment.
If a patient has uncontrolled asthma, the first step is not stem cells.
The first step is to ask why.
These questions are often more useful than jumping directly to advanced therapy.
For asthma alone, regenerative medicine remains a much more cautious and less established conversation. It should not be marketed as a cure. It should not replace standard asthma care.
If COPD features are also present, the discussion changes. But again, diagnosis comes first.
This happens more often than people think.
A patient brings reports from different years. One says asthma. Another says chronic bronchitis. Another says COPD. A newer one mentions emphysema. The patient is confused, and sometimes embarrassed by the confusion.
They should not be.
The lungs change over time. Medical understanding also changes over time. Some diagnoses are made quickly during an infection or emergency visit. Some are repeated for years without full re-evaluation.
I usually tell patients:
“Let us not fight with the old labels. Let us understand your lungs today.”
That means looking at the current condition.
This is more useful than simply asking which word was used first.
This part must be said plainly.
Hope is important. I see that every day. Patients with chronic breathing problems need hope because the disease can make life feel smaller.
But hope without honesty becomes dangerous.
The ethical place for regenerative medicine is different.
It may be considered as a supportive option in selected COPD or asthma-COPD overlap patients, especially where chronic inflammation, repeated flare-ups and reduced endurance remain important problems despite standard care.
That is a careful sentence.
And in medicine, careful sentences are often the most honest ones.
Some patients should not wait for an appointment about regenerative medicine.
They need urgent care.
Severe breathlessness at rest, blue lips or fingertips, confusion, chest pain, coughing blood, high fever with breathing difficulty, oxygen levels dropping below the advised range, or being unable to speak in full sentences are warning signs.
This may be a severe asthma attack, COPD exacerbation, infection, heart problem, blood clot or another emergency.
In that situation, the priority is not an advanced supportive treatment.
The priority is safety.
Breathing emergencies must be treated as emergencies.
I try to slow the conversation down.
Patients often want a direct answer:
“Doctor, is this asthma or COPD?”
“Can stem cells help?”
“Are exosomes good for my lungs?”
But lungs do not always answer quickly.
So I usually explain it like this:
Asthma is often a disease of sensitive airways.
COPD is often a disease of long-term airway and lung tissue damage.
Some patients have both patterns.
Treatment depends on which pattern is really present.
Then we look at the details.
If it is mainly asthma, we optimize asthma care.
If it is mainly COPD, we focus on COPD care, flare-up prevention and functional support.
If it is overlap, we individualize.
If regenerative medicine is considered, it must fit the diagnosis — not replace it.
This order is important.
Because the wrong treatment at the wrong time is not advanced medicine.
It is just confusion with a more expensive name.
Asthma and COPD are often confused because they share symptoms.
But they do not behave the same way.
Asthma usually changes more. COPD usually stays more. Asthma often reacts strongly to triggers. COPD often builds slowly and affects daily life in a more permanent way. Some patients have both, and those patients need especially careful evaluation.
Regenerative medicine may have a supportive role in selected COPD or asthma-COPD overlap patients, particularly when chronic inflammation, repeated flare-ups and reduced endurance are part of the disease picture.
But it is not a cure.
It is not a replacement for inhalers, oxygen, pulmonary rehabilitation or respiratory follow-up.
And it should never be discussed before the diagnosis is clear.
The better question is not only:
“Can regenerative medicine help my breathing?”
but:
“What kind of breathing disease do I really have?”

Yes. It is possible.
Sometimes the first diagnosis was not wrong. The lungs may simply look different years later. A patient can have asthma for a long time and later develop more fixed airway narrowing, especially after smoking, pollution, repeated infections, or many years of inflammation.
Sometimes the first label was just incomplete.
I usually tell patients not to get stuck on the old word. We need to look at the lungs today. How you breathe now, what the spirometry shows, how much the inhaler helps, whether oxygen drops, whether imaging shows emphysema — these are more useful than arguing with an old report.
By symptoms alone, usually you cannot.
Wheezing does not automatically mean asthma. Cough does not automatically mean COPD. Both diseases can make the chest tight. Both can make stairs difficult.
The pattern gives hints. Asthma often comes and goes. It may be worse with dust, pollen, cold air, exercise, infection, smoke, or strong smells. COPD is usually more constant. It enters daily life slowly. People stop walking fast, stop using stairs, stop doing things they used to do.
But we still need testing. Spirometry before and after bronchodilator medication is one of the most useful tests. Without that, we are mostly guessing.
Yes, and this is where many patients get confused.
Some people have asthma-like airways, but also COPD-like damage. They may wheeze, but they also have morning mucus. They may have allergy, but they also have a smoking history. Their inhaler helps, but never completely.
Not as the first step.
Most asthma patients need the basics checked properly first. Diagnosis. Inhaler technique. Triggers. Allergy. Sinus disease. Reflux. Infection history. Whether the medication is being used correctly. Whether it is actually severe asthma or something else pretending to be asthma.
There are good established treatments for asthma. Some severe cases may even need modern biologic medicines.
So I would not present regenerative medicine as a standard asthma treatment. That would not be honest.
Mostly in selected COPD or asthma-COPD overlap patients, and even there, only as a supportive option.
Not as a cure.
Stem cells and exosomes are interesting because COPD involves chronic inflammation, immune signaling, repeated flare-ups, and a lung environment that often remains irritated for years.
The realistic aim is not to grow a new lung. It is to support a calmer inflammatory environment and possibly help with stability, flare-up tendency, or daily tolerance.