Regenerative Medicine
Clinical insights by Dr. Tengiz Tkebuchava, MD, PhD
Patients who look into regenerative treatment for the hip or knee usually run into the same problem very quickly. They start with one question, but after a few minutes of reading, they suddenly have four. PRP, PRF, stem cells, exosomes. Everything sounds modern. Everything sounds regenerative. And everything starts to blur together.
That confusion is understandable.
Most people are not trying to become experts in biologic medicine. They are trying to understand what may actually help their joint. They want to know whether these options are truly different, whether one is better than the others, and whether any of them might help them avoid surgery.
The answer is not as simple as choosing the most impressive name. In real practice, these are not interchangeable products. They play different roles, and they are not chosen for the same reason.
From the outside, all four seem to belong in the same category. They are all mentioned in regenerative medicine. They are all associated with healing. They are all used in orthopedics. So naturally, patients assume they must be variations of the same idea.
But that is not really how it works.
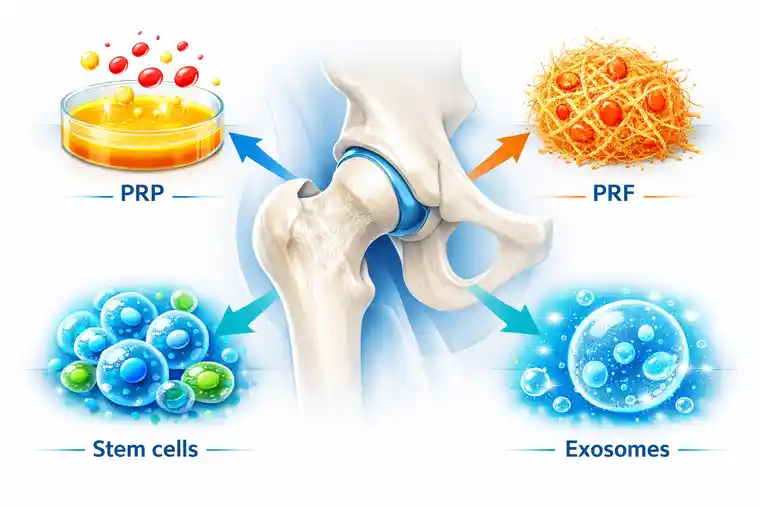
Some of these options come from the patient’s own blood. Some are used because of their signaling effect. Some are chosen for a broader regenerative purpose. And sometimes the most sensible plan is not one of them alone, but a combination.
That is why comparison matters. Not because patients need more complicated language, but because the wrong simplification creates the wrong expectations.
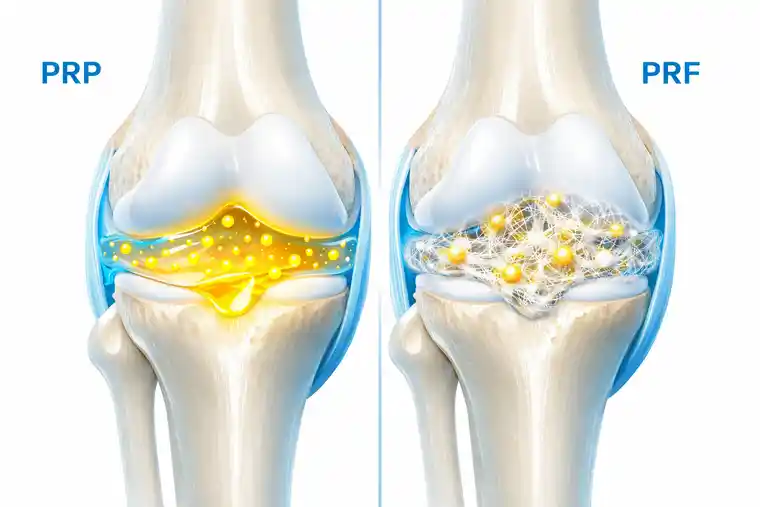
PRP stands for platelet-rich plasma. It is prepared from the patient’s own blood and then concentrated so that the platelet content becomes higher than usual. Those platelets contain growth factors, and that is why PRP is used in regenerative medicine.
In simple terms, PRP is often chosen when we want to support the healing environment of a joint using the patient’s own biological material.
This is part of why it became so popular. Patients like the idea that it comes from their own blood. It feels familiar, straightforward, and less foreign than other regenerative options they may read about online. In some cases, that matters psychologically as much as medically.
Still, PRP should not be described too dramatically. It is not a magic repair fluid, and it is not a replacement for cartilage in the literal sense. What it may do is support the biological conditions inside the joint so that irritation, inflammation, and recovery begin to move in a better direction.
This is where many patients start losing the thread.
PRF also comes from the patient’s own blood, so people assume it must be almost identical to PRP. But PRF has a different structure. It contains more fibrin, which means it behaves less like a simple liquid preparation and more like a biologically organized matrix.
That difference may sound technical, but clinically it matters.
PRF is often discussed when the goal is not only to deliver growth factors, but also to provide a more supportive regenerative setting. So even though PRP and PRF are related, they are not just two names for the same treatment. One is not automatically better than the other. They are simply different tools.
Patients do not need to memorize the laboratory details. They only need to understand one thing: if a doctor recommends PRF instead of PRP, it is not cosmetic wording. There is a reason for it.
The words stem cells naturally create strong expectations.
Patients hear them and immediately assume they must be the most powerful option in every case. Sometimes they even assume that if stem cells are available, everything else becomes second-best by definition. However, medicine is not that simple.
Stem cells are used because of their regenerative potential. In joint treatment, they may be selected when a broader biological strategy is needed, especially when the problem is more substantial and the treatment plan needs to go beyond a lighter supportive approach.
That does not mean every painful knee or hip automatically needs stem cells. It means stem cells may be more appropriate when the condition of the joint, the degree of cartilage loss, or the overall treatment goal calls for something more comprehensive.
In other words, stem cells are important. But they are not automatically the correct answer just because they sound like the most advanced option on the page.
Exosomes are probably the most misunderstood of the four.
Patients often place them mentally next to stem cells and assume they are simply a smaller or newer version of the same thing. They are not. Exosomes are not cells. They are signaling particles. Their role is connected to communication between cells rather than to being living cells themselves.
That sounds abstract at first, but the practical meaning is easier to understand than people expect.
A joint does not only depend on structure. It also depends on how the local tissue behaves, how cells respond, how inflammation is regulated, and how repair signals are carried. Exosomes are interesting because they may influence that signaling environment.
So when exosomes are used, the point is not that they “become” cartilage or replace tissue directly. Their role is more about supporting the communication that shapes healing.
This question comes up constantly, especially from patients who prefer treatment based on their own body.
If that is the main concern, PRP and PRF are usually the clearest examples because both are derived from the patient’s own blood. That makes them feel familiar and direct. Many patients find that reassuring.
Stem cells may also be autologous in some treatment models, but not always. In other cases, donor-based sources may be considered. Exosomes are usually understood less in terms of “is this from me?” and more in terms of what kind of biological signaling role they may have.
So yes, PRP and PRF are often the most straightforward answer when a patient asks for the most obviously autologous option.
But that still does not answer the deeper medical question, which is whether the most natural option is enough for the actual condition of the joint.
That is probably the most predictable question of all.
People want a ranking. They want PRP on one step, PRF on another, stem cells on top, and maybe exosomes somewhere in between. It would certainly make the conversation easier if medicine worked like that. But it usually does not.
A treatment is not strong in isolation. It is strong or weak in relation to the problem it is trying to solve.
In one patient, PRP may be a completely reasonable choice. In another, it may be too limited. In one joint, exosomes may add something very valuable. In another, stem cells may make more sense as the central strategy. Sometimes the real answer is not one option defeating the others, but several methods working together because the joint itself is dealing with more than one issue.
So I usually try to move patients away from the question “Which one is strongest?” and toward a better one: “Which one is right for my joint?”
That is the question that leads somewhere useful.
When choosing between PRP, PRF, stem cells, and exosomes, the actual condition of the joint matters more than the popularity of the product.
Cartilage quality matters. Inflammation matters. The stage of degeneration matters. Age matters. Activity matters. Previous treatment matters. And expectations matter too, because the best biological option on paper is still the wrong plan if it does not fit what the patient is realistically hoping to achieve.
Some patients mainly need a supportive push in the healing environment. Others need a broader regenerative concept. Some want only autologous options. Others are open to a wider range of biologic materials. Some cases are relatively early. Some are not.
That is why good regenerative medicine does not begin with a menu. It begins with assessment.
This is another place where patients are often surprised.
They expect the doctor to choose one winner and reject the rest. But a painful hip or knee is not always one clean problem. There may be inflammation, tissue stress, altered movement, poor local signaling, chronic overload, and cartilage wear all happening together. When that is the reality, one isolated method may not always be the most intelligent approach.
That is where combination treatment comes in.
A doctor may combine stem cells with exosomes because one contributes broader regenerative support while the other contributes signaling support. In another situation, PRP or PRF may be part of a treatment plan because an autologous element is useful. Supportive therapies such as ozone, red light, or shockwave may also be added if the goal is to improve the overall biological response of the tissue.
That is not done for show. It is done because joints are complex, and sometimes the best answer is not a single product but a better-built environment for healing.
If patients want the comparison in the simplest possible terms, this is often the clearest place to start.
PRP and PRF belong closer together because both are blood-based, autologous options. Stem cells and exosomes are different in character. Stem cells are considered for broader regenerative potential. Exosomes are valued for signaling.
That basic distinction already helps reduce a lot of confusion.
Once patients understand that PRP and PRF are not the same as stem cells, and exosomes are not the same as either of them, the conversation becomes much easier. Then we can stop comparing labels and start comparing what the joint may actually need.
Sometimes yes, but this question has to be handled honestly.
The goal of regenerative medicine is not to promise that no operation will ever be needed. That is not serious medicine. The real goal is to improve the condition of the joint enough that pain, function, and daily life move in a better direction, sometimes to the point that surgery can be postponed or, in selected patients, avoided.
Any of these options may play a role in that process depending on the case. For one patient, PRP may be enough at the right moment. For another, stem cells or exosomes may be more appropriate. For another, a combination may be the better path.
What matters is not winning a competition against surgery in theory. What matters is preserving joint function for as long as it remains medically realistic.
Patients often hope there is one hidden answer behind all these names. One best option. One treatment that makes the rest unnecessary.
In practice, that is usually not how medicine works.
I do not see PRP, PRF, stem cells, and exosomes as rivals. I see them as different biological tools. Each has a place. Each has limits. Each becomes useful only when matched properly to the problem in front of us.
That is why the most advanced treatment is not the one with the most fashionable name. It is the one chosen for the right reason.

There is no honest way to answer that with one word.
Patients often want a ranking, but these options are not chosen like medals. What works best depends on the joint itself. A mildly irritated joint may not need the same kind of treatment as one with more cartilage damage or more persistent inflammation. In some cases, PRP is enough. In others, stem cells or exosomes may make more sense. And sometimes the better result comes from combining methods rather than choosing only one.
So the real question is usually not which one is best in general, but which one fits the condition of the joint best.
PRP is more of a platelet-rich plasma preparation.
PRF contains more fibrin, so it behaves more like a healing matrix.
That may sound like a small difference, but in treatment planning it is not. PRP is often thought of more as a fluid concentrate of growth factors. PRF has a more structured character because of the fibrin. So even though both come from the patient’s own blood, they are not just two names for the same thing.
That is exactly why a doctor may choose one over the other depending on what kind of support the joint seems to need.
No.
Patients often assume they must be closely related because the two are mentioned together so often. But they are not the same. Stem cells are cells. Exosomes are something else. They are used for a different reason and they do not play the same role in treatment.
That is why choosing between them is not a matter of picking the newer or more advanced-sounding word. The question is what kind of support the joint actually needs.
PRP and PRF are the clearest examples of that.
Both are prepared from the patient’s own blood, so they are usually the most straightforward choice for patients who want an autologous treatment. Stem cells may also come from the patient in some treatment concepts, but not always. Exosomes are usually discussed less in terms of “from my own body” and more in terms of what role they may play in regenerative signaling.
So if using your own biological material is the main priority, PRP and PRF are often the first options patients ask about.
Yes, in some patients they can.
A painful hip or knee is not always dealing with one issue only. There may be cartilage wear, inflammation, overload, poor tissue signaling, and mechanical stress all at the same time. Because of that, some treatment plans are built around more than one regenerative method.
For example, one case may involve stem cells and exosomes together. Another may use PRP or PRF as part of a more autologous approach. The decision depends on what the joint seems to need, not on trying to use more products just for the sake of it.
When patients compare PRP, PRF, stem cells, and exosomes, they are usually trying to answer a very human question: what gives me the best chance to help this joint without rushing toward surgery?
The real answer depends on the joint itself.
PRP and PRF are often chosen when an autologous blood-based approach is preferred. Stem cells are considered when a broader regenerative strategy may be needed. Exosomes are valued for their signaling role and the way they may support the healing environment. In some cases, one of these options is enough. In others, the better decision may involve combining them.