Some parts of colorectal surgery look clear only after the case is over.
On video, the dissection may seem smooth. The plane opens at the right point. The vessels are controlled. The pelvis looks understandable. The stapler comes in at the right time. But during the operation itself, those decisions are not always that obvious.
Where exactly is the plane?
Is the exposure enough?
Should the surgeon continue laparoscopically, or is this the point to change the plan?
Is the tissue ready for stapling, or is the operation being pushed too quickly?
These are the questions that make advanced colorectal surgery different from simply knowing the steps of an operation.
The Advanced Laparoscopic Colorectal Surgery Cadaveric Masterclass will take place on 12–13 September 2026. The course is directed by Prof. Dr. Erdem Kınacı and Dr. İlyas Kudaş and is planned as a focused two-day training program for surgeons who want more structured exposure to advanced laparoscopic colorectal procedures.
The laparoscopic colorectal surgery course brings together theory, operative video discussion, cadaveric dissection and complication management. Its main subjects include complete mesocolic excision, total mesorectal excision, laparoscopic right hemicolectomy, left hemicolectomy, sigmoidectomy, splenic flexure mobilization and low anterior resection.
It is not a general introduction to laparoscopy. It is closer to a working session on anatomy, planes, instruments and decision-making.
Table of Contents
The Part of Colorectal Surgery That Is Difficult to Teach from Slides

Colorectal surgery depends heavily on anatomy, but not only in the way anatomy is learned from a drawing.
A surgeon needs to understand how the anatomy appears during dissection. The mesocolic plane is not just a term. The mesorectal plane is not just an illustration in a lecture. Vascular anatomy is not only something to identify after the specimen is out.
These structures guide the operation while it is happening.
In advanced laparoscopic colorectal surgery, this becomes even more important. The surgeon is working with a magnified view, but also with long instruments and limited tactile feedback. The screen may show the field clearly, but orientation can still be lost if the exposure is poor or the dissection moves away from the correct plane.
This is why the masterclass places anatomy at the center of the program.
The course reviews surgical and embryological anatomy of the colon and rectum, vascular anatomy, pelvic anatomy, CME and TME principles. But the purpose is not just to repeat anatomical information. The purpose is to connect anatomy with the practical choices a surgeon makes during the operation.
Where should the dissection start?
Which tissue layer should be respected?
How is the vessel approached safely?
When is the plane correct, and when is it only looking correct?
These are not small questions in colorectal surgery.
Advanced Laparoscopic Colorectal Surgery Masterclass at a Glance
📌 Format: Theory, video-based surgical approach, cadaveric dissection and complication management
📅 Duration: 2 days, 12–13 September 2026
📍 Location: Istanbul, Turkey
🧪 Training model: Step-by-step cadaveric dissection
👨⚕️ Supervision: Expert faculty guidance
🎓 Certificate: Certificate presentation at the end of the program
💳 Course fee: USD 2,750
✅ Included: Theoretical sessions, video-based surgical strategy, cadaveric practical sessions, complication management workshop, course evaluation, materials, meals, coffee breaks, on-site educational coordination and membership card
📞 Contact: For registration details and availability, our medical education coordination team is available by WhatsApp at +90 537 977 89 84.
A Laparoscopic Colorectal Surgery Course Built Around CME, TME and Real Operative Judgment
The masterclass focuses on procedures that require more than routine laparoscopic familiarity.
Complete mesocolic excision, or CME, is one of the main areas of the program. For right-sided colon surgery, CME is closely connected with oncologic discipline, central vascular ligation and the quality of the mesocolic plane. The operation is not only about removing the colon segment. It is about doing the dissection in a controlled and anatomically meaningful way.
Total mesorectal excision, or TME, brings another kind of challenge. Rectal surgery is performed in a narrow space, where the plane, the nerves, the distal transection and the anastomotic plan all matter. A small loss of orientation in the pelvis can change the difficulty of the operation very quickly.
The program also includes laparoscopic right hemicolectomy with intracorporeal anastomosis, left hemicolectomy or sigmoidectomy, splenic flexure mobilization and low anterior resection.
These are familiar words to colorectal surgeons. But familiarity with the names of the procedures is not the same as confidence in the details.
That is why the course is structured around step-by-step teaching rather than broad theoretical review.
What Happens Before the Cadaveric Lab
The first part of the masterclass begins with the details that shape the rest of the operation.
Operating room setup, patient positioning, port placement and ergonomics are discussed early in the program. These topics can sound basic, but in laparoscopic colorectal surgery they are often the difference between a comfortable operation and a difficult one.
A trocar placed badly can limit the whole dissection.
A poor patient position can make exposure harder.
Bad ergonomics can affect precision.
A stapler may be easy to fire, but difficult to position correctly.
The course also covers the safe use of energy devices and staplers. This is important because modern colorectal surgery depends on these tools, but tools do not replace surgical judgment. The surgeon still has to decide when the tissue is safe to divide, when the exposure is acceptable and when the plan needs to be changed.
After the theoretical sessions, the program moves into video-based surgical discussion. This part is not only about watching a clean case. A useful operative video shows the order of steps, but it also shows where decisions are made.
For example, in laparoscopic right hemicolectomy, the video discussion can help clarify the operative roadmap for CME and intracorporeal anastomosis. In left-sided surgery, it can show the logic of the medial-to-lateral approach, vascular control and splenic flexure mobilization. In low anterior resection, it can help participants follow the pelvic dissection and understand the steps before entering the cadaveric lab.
Video gives the map.
Cadaveric dissection gives the surgeon time to walk through it.
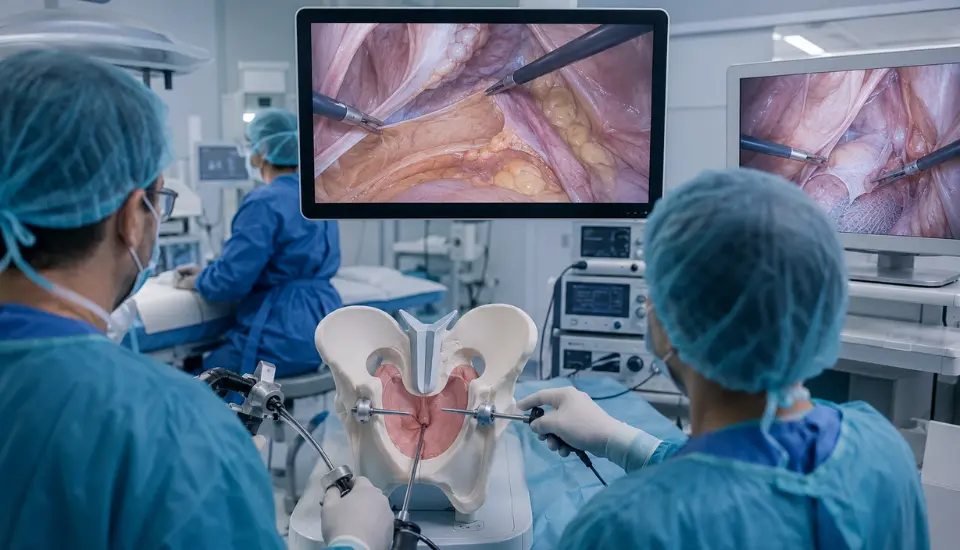
Why Cadaveric Dissection Matters in This Course

Cadaveric training has a different place in surgical education.
For advanced colorectal surgery, it offers something valuable: real anatomy, real spatial relationships and time to study the planes without the same pressure as the operating room.
In this masterclass, cadaveric dissection is not a short demonstration added to the end of a lecture day. It is one of the core parts of the course.
Participants work through selected steps of advanced laparoscopic colorectal procedures under supervision. The first cadaveric session focuses on CME with laparoscopic right hemicolectomy and intracorporeal anastomosis. The second day continues with left hemicolectomy or sigmoidectomy with splenic flexure mobilization, followed by laparoscopic low anterior resection with TME.
This gives the course a practical rhythm.
First, the anatomy is reviewed.
Then the operation is discussed on video.
Then the participant enters the cadaveric lab and works through the dissection step by step.
That sequence is important. It gives participants a chance to connect what they know with what they do.
In colorectal surgery, that connection is where much of the learning happens.
Right Hemicolectomy and Intracorporeal Anastomosis
The first cadaveric practical session focuses on laparoscopic right hemicolectomy with CME and intracorporeal anastomosis.
This part of the course is especially useful because right-sided colon surgery involves both oncologic dissection and reconstructive technique. The surgeon has to understand the mesocolic plane, central vascular control and the technical steps of intracorporeal anastomosis.
Intracorporeal anastomosis also requires a certain level of laparoscopic organization. The bowel has to be handled carefully. The stapler has to be introduced and used with control. The orientation of the bowel matters. The closure step must be planned, not improvised.
During a regular operation, these details may pass quickly. In a cadaveric setting, they can be slowed down and examined more deliberately.
That is one of the main strengths of this type of masterclass. It gives surgeons space to study the operation, not just watch it.
Left Hemicolectomy, Sigmoidectomy and Splenic Flexure Mobilization
Left-sided colorectal surgery has its own difficulties.
A left hemicolectomy or sigmoidectomy may be a familiar procedure, but the difficulty can change depending on the anatomy, exposure, body habitus, adhesions or the need for splenic flexure mobilization.
The splenic flexure is a good example. It is often discussed as a step, but in practice it can become one of the more demanding parts of the operation. The surgeon needs to understand the attachments, the relationship to the transverse colon, the descending colon, the omentum and the surrounding structures. Good exposure matters. The direction of traction matters.
In the masterclass, left-sided surgery is approached through theory, video-based planning and cadaveric dissection. This allows participants to review the medial-to-lateral approach, vascular control and mobilization strategy before practicing the steps in the lab.
For surgeons who want to become more confident in advanced laparoscopic colorectal work, this kind of focused repetition can be useful. It is not about learning a shortcut. It is about understanding the operation more clearly.
TME and Low Anterior Resection
The low anterior resection section of the course focuses on TME.
This is one of the most important parts of advanced colorectal training because rectal surgery requires precision in a confined anatomical space. The pelvis does not give much room for careless movement. The mesorectal plane has to be followed. Nerve preservation has to remain in mind. The distal transection and anastomotic plan need careful judgment.
In theory, the steps of TME can be explained clearly. In practice, the operation demands orientation, patience and good exposure.
The cadaveric session allows participants to work through the pelvic dissection in a controlled educational setting. This can help surgeons better understand how the plane feels visually, how the dissection progresses and where the operation becomes more sensitive.
A good TME is not only about completing the dissection. It is about respecting the anatomy throughout the dissection.
Complications Are Not a Separate Topic
One of the important parts of the course is complication management.
In advanced colorectal surgery, complication management is part of the operation itself. The surgeon is constantly making safety decisions.
Bleeding may occur.
The anatomy may not be clear.
The tissue may not behave as expected.
The anastomosis may carry risk.
The laparoscopic approach may no longer be the safest option.
For that reason, the masterclass includes conversion criteria, intraoperative troubleshooting and anastomotic leak management principles.
Conversion is especially important to discuss properly. It should not be presented as failure. Sometimes conversion is the correct surgical decision. What matters is recognizing the point where continuing laparoscopically may create more risk than benefit.
Anastomotic leak management is also included because colorectal surgery does not end when the anastomosis is created. The surgeon has to think about risk, prevention, recognition and management.
By including these topics, the course becomes more realistic. It does not only show the operation when everything is going well.
Who Is This Masterclass For?
This laparoscopic colorectal surgery course is mainly intended for surgeons who already have a foundation in laparoscopic surgery and want more focused training in colorectal procedures.
It may be suitable for colorectal surgeons, general surgeons with an interest in colorectal surgery, surgeons involved in oncologic colorectal procedures, surgical residents, fellows and surgeons who want to strengthen their approach to CME, TME, laparoscopic colectomy and low anterior resection.
It may also be useful for surgeons who want more cadaveric practice in anatomical dissection, splenic flexure mobilization, intracorporeal anastomosis and complication decision-making.
The course is advanced. That does not mean every participant is expected to already be an expert in all of these procedures. But it does mean the program is not designed as a first step into laparoscopy. Participants should ideally have basic laparoscopic knowledge and a serious interest in colorectal surgery.
For the right participant, the value of the course is not only the list of procedures. It is the chance to study advanced colorectal surgery with a more structured eye.
A Two-Day Program with a Clear Progression
The program is organized over two days.
The first day begins with registration, opening and orientation. The morning is dedicated to theoretical sessions, including operating room setup, patient positioning, port placement, ergonomics, surgical and embryological anatomy, CME, TME, laparoscopic right hemicolectomy, left-sided colorectal surgery, low anterior resection and complication management.
After lunch, the course moves into the cadaveric laboratory. Participants receive a briefing on safety rules, station allocation and procedure objectives. The afternoon then continues with video-based surgical planning and the first cadaveric practical session on CME with laparoscopic right hemicolectomy and intracorporeal anastomosis.
The second day is more practice-oriented. It includes cadaveric practical sessions on left hemicolectomy or sigmoidectomy with splenic flexure mobilization and laparoscopic low anterior resection with TME. Later in the day, the program continues with a complication management workshop, course evaluation and certificate presentation.
The structure is compact, but it is not random. Each part prepares the next one.
Theory prepares the video discussion.
Video discussion prepares the cadaveric dissection.
Cadaveric dissection makes the anatomy more practical.
Complication management brings the focus back to safety and judgment.
A Focused Training Experience in Advanced Colorectal Surgery
Advanced laparoscopic colorectal surgery is not only about being able to use laparoscopic instruments.
It requires anatomical orientation, technical discipline and the ability to make safe decisions when the operation becomes difficult. CME, TME, splenic flexure mobilization, intracorporeal anastomosis and low anterior resection all require this kind of thinking.
The Advanced Laparoscopic Colorectal Surgery Cadaveric Masterclass 2026 is designed around that need.
For surgeons who want to work more closely on advanced colorectal procedures, the course offers a structured opportunity to review the principles, study operative strategy, practice cadaveric dissection and discuss complication management under faculty guidance.
For doctors who want to follow medical education opportunities, treatment updates and healthcare developments in Turkey, MedClinics also shares regular insights through its Medical News & Blog’s section.
FAQ: Advanced Laparoscopic Colorectal Surgery Cadaveric Masterclass
What is the Advanced Laparoscopic Colorectal Surgery
Cadaveric Masterclass?
It is a two-day laparoscopic colorectal surgery course focused on advanced techniques, cadaveric dissection, video-based surgical planning and complication management.
When will the masterclass take place?
The masterclass will take place on 12–13 September 2026.
Which procedures are included in the course?
The program includes CME, TME, laparoscopic right hemicolectomy, intracorporeal anastomosis, left hemicolectomy or sigmoidectomy, splenic flexure mobilization and laparoscopic low anterior resection.
Is this a hands-on course?
Yes. The course includes step-by-step cadaveric dissection sessions in addition to lectures and video-based surgical discussion.
Who is the course suitable for?
It is mainly suitable for colorectal surgeons, general surgeons, surgical residents, fellows and surgeons with a laparoscopic background who want more focused training in advanced colorectal surgery.
Why does the course include cadaveric dissection?
Cadaveric dissection allows participants to study real anatomical structures, follow surgical planes and practice selected steps of advanced colorectal procedures in a supervised educational setting.
Does the masterclass include complication management?
Yes. The laparoscopic colorectal surgery course includes conversion criteria, intraoperative troubleshooting and anastomotic leak management principles.
Will participants receive a certificate?
Yes. The program includes course evaluation, feedback and certificate presentation at the end of the masterclass.