Clinical Insights from Prof. Dr. Serdar Kabataş, MD, PhD (C)
COPD Exacerbations: Why Flare-Ups Matter More Than a Bad Breathing Day
Many COPD patients say:
“I had a bad week.”
“My breathing suddenly got worse.”
“I needed the rescue inhaler more.”
That is usually how it begins.
Not always dramatically.
Not always with an ambulance.
Not always with fever.
Sometimes a COPD flare-up starts quietly. A little more cough. A little more mucus. A little more breathlessness. The patient waits. They think it will pass.
But in COPD, waiting can be risky.
A flare-up is not only a temporary worsening of symptoms. It can be a turning point. It can push the lungs into a period of increased inflammation, increased airway narrowing, increased mucus, and sometimes incomplete recovery.
This is why I take COPD exacerbations seriously.
Because the patient may call it “a bad few days.”
But the lungs may experience it as another injury.
Table of Contents
What Is a COPD Exacerbation?
A COPD exacerbation means the patient’s usual respiratory symptoms suddenly become worse than normal.
- More breathlessness.
- More cough.
- More sputum.
- More wheezing.
- More chest tightness.
- More fatigue.
- Sometimes fever.
- Sometimes oxygen levels dropping.
Some flare-ups are mild and can be managed early. Others require antibiotics, steroids, oxygen adjustment, emergency evaluation or hospitalization.
The important part is the change from the patient’s usual baseline.
Every COPD patient has a different normal.
One patient may cough every morning but walk well.
Another may have little cough but become breathless with small effort.
Another may already use oxygen and notice small changes very quickly.
So the question is not only:
“Are you breathless?”
We need to ask if the patient is more breathless than usual.
That difference matters.
Why COPD Flare-Ups Happen
COPD lungs are vulnerable lungs.
The airways are already narrowed. The lining may already be irritated. Mucus clearance may already be weaker. The immune system may already be on alert. The breathing muscles may already be working harder than they should.
Then something comes on top of that.
- A viral infection.
- A bacterial infection.
- Cold weather.
- Air pollution.
- Cigarette smoke.
- Dust.
- Chemical fumes.
- Strong smells.
- Poor sleep.
- Wrong inhaler technique.
- Missed medication.
- Heart strain.
- Reflux.
- Sometimes no clear trigger at all.
Patients often ask me, “Why did it happen? I did not do anything different.”
Sometimes they are right.
In COPD, the lungs can react strongly to things that would not affect a healthy person very much. A simple cold can become a chest infection. A polluted day can become a week of wheezing. Cold air can tighten the airways and make mucus harder to clear.
The lung has less reserve.
That is the problem.
When reserve is low, small triggers can create large consequences.
What Happens Inside the Lungs During a Flare-Up
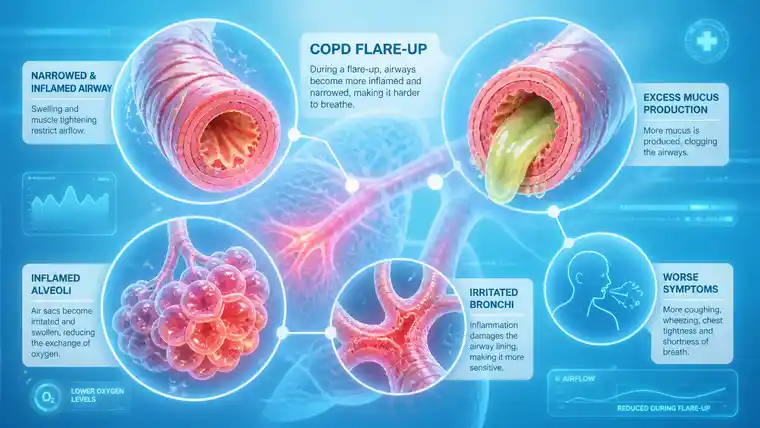
During a COPD flare-up, the lungs become more inflamed.
The airway lining swells. Mucus often increases. The airways narrow further. Air becomes trapped. Breathing out becomes harder. Then breathing in becomes harder too, because the lungs have not fully emptied.
This is why patients describe the feeling of air being stuck.
They may say:
“I cannot empty my lungs.”
“I breathe, but it does not feel useful.”
“I need to sit forward.”
“I cannot finish a sentence.”
“I feel tired from breathing.”
That tiredness is real.
During a flare-up, breathing becomes work. Muscles in the chest, neck and shoulders may join the effort. The patient may sleep poorly. Eating may become difficult. Anxiety may rise, not because the patient is weak, but because air feels uncertain.
And when air feels uncertain, the whole body reacts.
A COPD exacerbation is not only a lung event. It affects the whole person.
Why Some Patients Do Not Recover Fully
This is very important. One may recover completely, other may not.
They say:
“I am better than last week, but not like before.”
“I need more pauses now.”
“I lost confidence.”
“I still feel weak.”
“I thought I recovered, but walking is different.”
This is why repeated exacerbations matter. They can reduce functional reserve. They can lead to more inactivity. Inactivity weakens muscles. Weak muscles make breathlessness worse. Worse breathlessness makes the patient move even less.
A cycle begins.
- Flare-up.
- Recovery.
- Less movement.
- More weakness.
- More breathlessness.
- More fear.
- Another flare-up.
Not every patient follows this path, but many do.
And once the patient begins living around the fear of the next flare-up, COPD becomes more than a diagnosis.
It becomes a limit on daily life.
Why COPD Flare-Ups Can Speed Up Decline
COPD usually progresses slowly.
But flare-ups can interrupt that slow pattern.
Each significant exacerbation can increase inflammation and stress in the lungs. The airway environment becomes more unstable. The patient may need systemic medications. Hospitalization may become necessary. Oxygen levels may drop. The heart may be strained. Sleep and nutrition may suffer.
Preventing flare-ups is not only about avoiding hospital visits.
It is about protecting the patient’s remaining lung reserve.
In COPD, reserve is precious.
That is why I ask about flare-ups very carefully.
Not only:
“Have you been hospitalized?”
But also:
“How many times did your breathing worsen this year?”
“Did you need antibiotics?”
“Did you need steroids?”
“Did you stay in bed?”
“Did you recover fully?”
“Are you walking less since then?”
These answers often tell me more than one number on a report.
COPD Exacerbation Symptoms Patients Should Watch For
A flare-up usually announces itself.
Not always loudly, but it gives signs.
- More breathlessness than usual.
- More frequent rescue inhaler use.
- More cough.
- More mucus.
- A change in mucus color or thickness.
- More wheezing.
- Chest tightness.
- Fever or chills.
- More fatigue.
- Poor sleep.
- Less ability to do normal activities.
- Oxygen levels lower than usual, if the patient monitors them.
Patients should know their own baseline.
I often tell patients:
Do not only watch the symptom.
Watch the change.
COPD care becomes safer when patients know what is normal for them and what is not.
When a COPD Flare-Up Needs Urgent Help
Some symptoms should not wait.
A COPD patient should seek urgent medical care if there is severe breathlessness at rest, blue lips or fingertips, confusion, chest pain, coughing blood, high fever, oxygen levels dropping below the advised range, or inability to speak full sentences.
Worsening despite rescue medication is also important.
So is sleepiness or mental confusion.
Families should pay attention here.
Unusual quietness can be a warning sign.
A breathless patient may stop complaining because speaking itself becomes effort.
That is not reassurance.
That can be danger.
Why Patients Sometimes Delay Treatment
Many COPD patients wait too long before asking for help.
Not because they are careless.
Often the opposite.
They do not want to be a burden or go to the hospital again.
They hope it will pass.
They think they should be stronger.
This delay can make the flare-up harder to control.
Early treatment may prevent a mild exacerbation from becoming a severe one. It may reduce the need for emergency care. It may protect recovery.
Patients should not feel guilty about seeking help early.
COPD is unpredictable. A flare-up can change quickly.
A patient who knows their warning signs and acts early is not overreacting.
They are protecting their lungs.
What Doctors Usually Look For During an Exacerbation
When a COPD patient worsens, we need to understand why.
- Is it viral?
- Bacterial?
- Air pollution?
- Heart-related?
- Pulmonary embolism?
- Pneumonia?
- Poor inhaler use?
- Medication interruption?
- Another disease imitating a COPD flare-up?
Not every worsening is simple COPD.
That matters.
A patient with COPD can also have heart failure. Pneumonia. Blood clot. Anemia. Arrhythmia. Anxiety. Sleep-related breathing problems. Medication side effects.
The goal is to recover well and prevent the next one.
How Flare-Ups Affect the Heart and the Whole Body
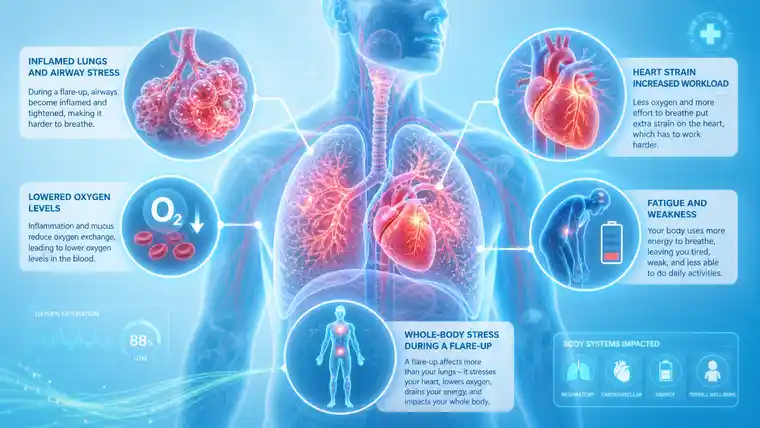
COPD exacerbations are not isolated lung events.
During a flare-up, oxygen may drop. Carbon dioxide may rise in some patients. The heart may work harder. Blood pressure and heart rhythm can be affected. Sleep becomes poor. Appetite decreases. Muscles weaken. Inflammation may spread beyond the lungs.
This is why older patients or patients with heart disease may become fragile during an exacerbation.
Sometimes the breathing problem and heart problem worsen each other.
The patient says, “It is my lungs.”
Maybe.
But the heart may also be under stress.
That is why COPD care must not be too narrow.
The lungs are central, but the whole body is involved.
A flare-up can reveal problems that were already there but hidden.
Preventing COPD Exacerbations
Prevention is not one thing.
It is many small things done consistently.
- Using inhalers correctly.
- Taking maintenance treatment as prescribed.
- Avoiding smoke and polluted air when possible.
- Getting recommended vaccinations.
- Treating infections early.
- Staying active within safe limits.
- Joining pulmonary rehabilitation when appropriate.
- Managing reflux, sleep apnea or heart disease.
- Maintaining nutrition.
- Knowing when to call the doctor.
- Having an action plan.
Patients often look for one big solution.
But COPD is usually managed by protecting many small margins.
- A correct inhaler technique may reduce risk.
- A vaccine may prevent an infection.
- Pulmonary rehabilitation may improve endurance.
- Recognizing early mucus change may lead to earlier treatment.
- Avoiding cold air exposure may prevent a difficult week.
These things sound simple.
They are not always easy.
But they matter.
Why Pulmonary Rehabilitation Matters After a Flare-Up
After a COPD flare-up, many patients rest.
Rest is necessary at first.
But too much rest becomes another problem.
Muscles lose strength quickly. The patient becomes afraid of breathlessness. Walking distance shrinks. The next activity feels harder. Then the patient avoids activity again.
This is how deconditioning begins.
Pulmonary rehabilitation helps break that cycle.
It does not repair destroyed lung tissue. But it trains the body to use what remains more efficiently. It helps breathing technique, muscle strength, endurance and confidence.
Patients sometimes say:
“How can exercise help if my lungs are damaged?”
The answer is that COPD is not only about lungs.
The muscles, heart, breathing pattern and confidence all matter.
A stronger body tolerates COPD better than a weaker body.
That is why recovery after a flare-up should not only mean “the infection is gone.”
It should mean:
Can the patient walk again?
Can they sleep?
Can they eat?
Can they return to their previous routine?
Do they trust their breathing again?
Where Regenerative Medicine Enters the Discussion
Regenerative medicine enters this conversation because COPD exacerbations are closely linked to inflammation, immune signaling and poor recovery.
Stem cells and exosomes are being studied because they may influence the inflammatory environment in chronic lung disease.
But this must be said carefully.
Regenerative medicine does not treat an acute emergency flare-up.
Stabilize first.
Only later, when the patient is stable, can we discuss long-term supportive strategies.
In selected COPD patients, regenerative medicine may be considered because the goal is to calm excessive inflammatory signaling, support the remaining lung environment, and possibly help reduce the burden of repeated inflammatory cycles.
That is not the same as curing COPD.
It is not rebuilding destroyed alveoli.
It is not replacing inhalers, oxygen, antibiotics, steroids, rehabilitation or respiratory follow-up.
It is a supportive discussion.
A careful one.
And only for the right patient at the right time.
What Regenerative Medicine Cannot Do During a Flare-Up
This needs to be very clear.
If a COPD patient is in the middle of a significant exacerbation, regenerative therapy is not the emergency treatment.
- It will not open the airways immediately.
- It will not replace rescue medication.
- It will not treat pneumonia.
- It will not correct dangerously low oxygen.
- It will not replace hospitalization when hospitalization is needed.
I say this because patients sometimes search for advanced treatments when they are already in crisis.
That is not the moment.
First we control the acute situation. We treat infection if present. We support oxygen. We reduce airway inflammation with appropriate medication. We monitor the patient. We protect the heart and the whole body.
Then, after recovery, we ask a different question:
- Why did this flare-up happen?
- Can we reduce the risk of another one?
- Is the current treatment plan enough?
- Is there a chronic inflammatory pattern that remains active?
- Is the patient a candidate for supportive regenerative strategies?
- Timing matters.
In medicine, the right treatment at the wrong time can become the wrong treatment.
Who May Need a Deeper Evaluation After Repeated Flare-Ups
Some COPD patients should be evaluated more deeply after exacerbations.
Especially patients who:
- have two or more flare-ups in a year,
- need frequent antibiotics or steroids,
- recover slowly after infections,
- lose walking distance after each episode,
- have oxygen levels dropping,
- have repeated hospital visits,
- have increasing mucus,
- or feel they never return to baseline.
These patients may have an unstable disease pattern.
Sometimes the problem is undertreated COPD. Sometimes inhaler technique is poor. Sometimes there is bronchiectasis, chronic infection, heart disease, reflux, sleep apnea, aspiration risk or immune weakness. Sometimes the patient is exposed to dust, smoke or pollution without realizing how much it matters.
Repeated flare-ups are a signal.
They tell us the lungs are not stable.
The answer is not always more medication. Sometimes it is better diagnosis, better prevention, better rehabilitation, better infection control, or better patient education.
And sometimes, once all of that is understood, supportive regenerative medicine may be discussed.
But not before the basics are clear.
How I Explain Flare-Ups to Families
Families often ask what they should watch for.
I tell them:
Watch the change.
If the patient sleeps sitting up, something is different.
If they stop eating because breathing is too much work, that matters.
Families sometimes see the flare-up before the patient admits it.
Not because the patient is hiding the truth.
Because COPD patients adapt.
They are used to discomfort. They normalize symptoms that other people would find alarming.
A family member may say:
“You were not like this last week.”
That sentence can be clinically useful.
It tells us there has been a change.
Final Thought: Preventing the Next Flare-Up
COPD exacerbations are not just interruptions.
They can change the course of the disease.
A flare-up may pass, but the patient may not fully return. Walking may become shorter. Sleep may become worse. Confidence may become smaller. The fear of the next episode may remain.
That is why every exacerbation should teach us something.
- What triggered it?
- Was treatment started early enough?
- Did the patient recover fully?
- Was oxygen affected?
- Is the inhaler plan correct?
- Is rehabilitation needed?
- Is infection prevention enough?
- Is chronic inflammation still active?
COPD care is not only about treating today’s symptoms.
It is about protecting tomorrow’s breathing.
Regenerative medicine may have a supportive role in selected stable patients, especially when chronic inflammation and repeated flare-ups remain part of the pattern. But it belongs after diagnosis, after stabilization, and beside standard COPD care.
Not instead of it.
The goal is simple, but important:
fewer bad weeks,
better recovery,
more stable breathing,
and a little more space in daily life.
For a COPD patient, that little space can mean a lot.
Frequently Asked Questions

How do I know if this is just a bad day or a real COPD flare-up?
I usually ask patients to compare it with their own normal. Not with another patient.
Not with a textbook. With themselves.
Are you more breathless than usual?
Are you using the rescue inhaler more?
Is the mucus different?
Are you walking less than last week?
Are you sleeping worse because of breathing?
If the answer is yes, especially if things are not settling, then it may be more than a bad day.
Why does a simple cold become so serious with COPD?
Because COPD lungs have less reserve.
A healthy person may get a cold and feel tired for a few days. A COPD patient may get the same virus, but the airways react more strongly. Mucus increases. Breathing becomes harder. Air gets trapped. Recovery takes longer.
The trigger may be small.
The reaction is not.
I recovered from the flare-up. Why do I still feel weaker?
This happens often. The infection or flare-up may be over, but the body has not fully recovered. During those days, breathing was hard work. Sleep was poor. Movement was less. Muscles lost strength. Confidence may also have been shaken.
So recovery is not only about the cough becoming better.
It is also about walking again, sleeping better, eating normally and trusting your breathing again.
Should I wait before calling the doctor?
Not if the change is clear.
Many COPD patients wait because they do not want to bother anyone. I understand that. But early help can sometimes prevent a small flare-up from becoming a hospital problem.
If breathlessness is clearly worse, oxygen is lower than usual, mucus has changed, fever appears, or rescue medication is needed much more often, it is better to ask early.
Can regenerative medicine help with COPD flare-ups?
It should not be seen as treatment for an active flare-up.
During a serious flare-up, the priority is standard medical care: oxygen if needed, bronchodilators, infection treatment, steroids when appropriate, and sometimes hospital support.
Regenerative medicine is a different conversation. It may be discussed later, when the patient is stable, especially if chronic inflammation and repeated flare-ups remain part of the disease pattern. But it is supportive. Not a cure. Not an emergency treatment.