
Clinical Insights by Prof. Dr. Serdar Kabataş, MD, PhD (C)
Clinical Perspective on Chronic Kidney Disease
I’m Prof. Dr. Serdar Kabataş, and I have worked in medicine for more than two decades. In neurosurgery, some conditions demand immediate action. Trauma does. Hemorrhage does. A spinal cord injury does.
Chronic kidney disease stem cell therapy is usually not the phrase patients arrive with first.
They come differently.
A patient notices swelling and ignores it for a while. Another is told that the blood pressure has been difficult to control for too long. Another feels tired, but not in a dramatic way. Just persistently. Quietly. Enough to change daily life, but not enough to force a decision in one day.
That quietness is part of what makes CKD so difficult.
I remember a patient who did not ask whether his kidneys could be cured. He asked whether he still had time. Time before dialysis. Time before life had to be reorganized around hospital visits, restrictions, and uncertainty.
That is usually the real question.
Because chronic kidney disease is not experienced as a single event. It is experienced as narrowing. Patients adapt. Then they adapt again. Families do the same.
From a medical perspective, CKD is not only about declining filtration. It is also about tissue that remains under chronic stress. Inflammation does not fully switch off. Repair is incomplete. Over time, useful tissue is replaced by scar tissue. That is one reason regenerative medicine entered this discussion at all. CKD is broadly understood as long-term kidney damage or reduced kidney function, and it often progresses silently in the earlier stages.
Not because the problem is simple.
Because it is not.
And if the disease is still active at a cellular level, the next question follows naturally: can we support the tissue before too much has been lost?
That is where a serious discussion begins.
Table of Contents
Chronic Kidney Disease Often Stays in the Background for Too Long
One of the most frustrating things about CKD is that patients may feel almost normal while the disease is already present.
That happens more often than people expect.
Many cases are first discovered through blood and urine testing, not because the patient suddenly feels ill. NIDDK notes that many people in the early stages have no symptoms, and for many, testing is the only way CKD is found.
So from the patient’s side, the diagnosis can feel sudden.
From the kidney’s side, it usually is not.
The disease has often been progressing in the background for quite some time.
The kidneys do more than most people think about in daily life. They help remove waste, regulate fluid, balance minerals, and contribute to blood pressure control. When they begin to struggle, the body can compensate for a while. That is one reason CKD can remain unnoticed longer than patients expect.
How CKD Usually Begins
In everyday practice, the most common causes are still diabetes and high blood pressure. These are the main reasons for chronic kidney disease in adults.
But patients rarely arrive with a story that is that clean.
Someone says, “My kidneys were damaged by diabetes,” and that may be true. But often there is more behind it. Years of hypertension. Weight gain. Vascular strain. Inconsistent check-ups. Sometimes medication exposure. Sometimes long periods where the disease simply did not feel urgent enough to change behavior.
That matters because CKD often builds layer by layer.
And once several layers are there, slowing it becomes harder.
Chronic Kidney Disease Stages: Why the Pattern Matters Too
Patients focus on the stage, and understandably so. Stage 2 sounds manageable. Stage 4 sounds frightening.
But stage alone never tells the whole story.
A single kidney number never tells the whole story.
We look at eGFR, a lab-based estimate of how much filtering capacity the kidneys still have (estimated Glomerular Filtration Rate). In general, the lower the eGFR, the weaker the kidneys are functioning. But we also look at albumin in the urine. Together, these two findings give a much more honest picture of risk.
A short summary is enough here.
- Stage 1 means kidney damage is present, but filtration may still look near normal.
- Stage 2 means mild loss of function.
- Stage 3 means moderate loss of function. This is often the stage where patients begin asking more practical questions about what comes next.
- Stage 4 means severe reduction.
- Stage 5 means kidney failure or near-kidney-failure, when dialysis or transplantation may enter the discussion.
But the stage is only one part of the picture.
A patient with stable stage 3 disease is not in the same position as a patient whose stage 3 disease is actively moving in the wrong direction every few months. The label may be the same. The reality is not.
Why CKD Progresses
This is the point many articles oversimplify.
The kidney does not simply “wear out.”
It is pushed.
Part of that pressure comes from the original cause, whether diabetes, hypertension, immune injury, or something else. But part of it comes from the kidney’s own response to injury. Inflammation persists. Fibrosis follows. Over time, healthy tissue is gradually replaced by scar tissue. KDIGO’s current framework and recent review literature both describe CKD as a disease shaped by ongoing injury, inflammatory activity, and progressive remodeling or scarring.
Patients usually understand fibrosis the moment it is explained plainly.
Scar tissue is not recovering tissue.
It is tissue that has already lost ground.
And once scarring dominates, medicine becomes more limited. That is why timing matters. Earlier disease leaves more room to work with. Advanced fibrosis leaves much less.
Why Chronic Kidney Disease Stem Cell Therapy Is Being Discussed
Stem cell therapy is being discussed because chronic kidney disease is not purely a structural problem.
It is also a signaling problem.
There is ongoing inflammatory activity. There is microvascular stress. There are fibrotic pathways that stay switched on. Mesenchymal stem cell approaches have drawn attention because their potential effect may come less from “becoming new kidney tissue” and more from influencing this hostile biological environment. Recent review papers describe these immunomodulatory and paracrine effects as one of the main reasons the field remains scientifically interesting.
That is the real point.
Many patients hear “stem cells” and imagine direct rebuilding. The actual scientific discussion is more restrained than that. The hope is that certain regenerative therapies may calm some of the biology that keeps the kidneys under pressure.
That is not the same as a cure.
But it is also not nothing.
How Treatment May Be Given
If stem cell or exosome treatment is discussed for CKD, patients usually want to know how it is actually given.
Sometimes it is administered through a vein, which means intravenously.
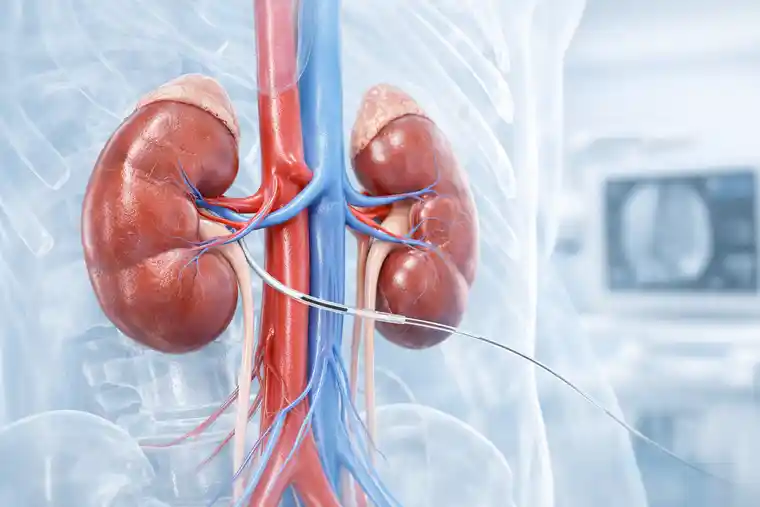
In some cases, however, a more targeted method is used. A very thin catheter can be guided under imaging into the vessels supplying the kidneys, so that the treatment reaches the renal circulation more directly. When this route is chosen, it should be performed by an experienced interventional radiologist. Current interventional radiology reviews describe trans-arterial delivery as one of the key targeted routes for cell therapy, and recent kidney disease reports have described renal intra-arterial infusion as feasible in selected settings.
The important point is not to make the procedure sound more dramatic than it is. The route of delivery should simply reflect the treatment plan, the anatomy, and the experience of the medical team.
Can Stem Cell Therapy Help CKD?
Possibly in selected patients.
That is the honest answer.
There are encouraging preclinical findings. There are also small human studies. Some report changes in inflammatory markers or kidney-related measures.
So the balanced answer is this:
The biology is interesting.
The clinical certainty is still limited.
For patients, that distinction matters. It determines whether a therapy is being discussed as careful support or being oversold as rescue.
Standard Kidney Care Still Comes First
This should not be a side note.
Any serious conversation about regenerative therapy has to begin with standard CKD care. It remains important to control blood pressure, prevent diabetes and reduce albuminuria.
In practical terms, that means something simple.
If blood pressure is uncontrolled, diabetes is poorly managed, medication is inconsistent, and follow-up is irregular, then no regenerative treatment is being asked to support the kidneys. It is being asked to compensate for ignored basics.
That is not a serious plan.
The clinics worth trusting are usually the ones that say this directly.
Which Chronic Kidney Disease Patients May Still Have a Meaningful Window?
The label may be the same, but the biology often is not.
One patient still has enough kidney function left that preservation is a meaningful goal. Another has already reached a point where scarring is advanced, the kidneys are small on imaging, and the disease has been shaping the body for a long time.
Those two patients should not be promised the same thing.
That is not harsh. It is simply clinical reality.
The first patient may justify a discussion about slowing progression.
The second often needs a more modest conversation. Preservation. Preparation. Quality of life. Avoiding false hope.
Two kidneys can share the same diagnosis and still be at very different points biologically.
That is why selection matters so much.
Diabetic Kidney Disease Matters More Than Many Patients Think
Diabetes is not just one cause among many. It is one of the major reasons CKD develops in the first place. NIDDK continues to describe diabetes as one of the two leading causes of chronic kidney disease.
It is also one of the most relevant settings for regenerative research.
The reason is not complicated. Diabetic kidney disease brings together several of the processes that make CKD hard to treat: metabolic stress, vascular damage, inflammation, and fibrosis.
That combination makes it one of the clearest examples of why regenerative approaches are being explored.
Whether those approaches will translate into consistent long-term benefit is still not fully answered.
But it is one of the key areas worth watching.
Where Exosomes Fit In

Exosomes are often mentioned together with stem cells, and sometimes too quickly.
The simplest way to think about them is this: they are part of cellular communication. Tiny messengers. Signals moving from one cell to another.
That is why researchers care about them in CKD. Much of the disease process is driven by signaling that has gone wrong long before the kidney reaches end-stage failure.
So yes, exosomes belong in the scientific discussion.
But they should not dominate it.
For most patients, the more important point is not the terminology. It is whether the treating physician can explain clearly what is established, what is emerging, and what is still more hope than evidence.
That matters much more than sounding advanced.
What Patients Can Realistically Hope For
This is usually the most human part of the consultation.
Most patients are not secretly waiting for a miracle. What they usually want is more ordinary than that.
Time.
Stability.
A slower decline.
A better year than the last one.
That is why regenerative therapy, if it is discussed honestly, should be framed around preservation rather than cure.
For a selected patient, the best realistic outcome may be slower progression, more stability in follow-up, or a treatment plan that tries to protect function rather than only document its loss.
That may not sound dramatic.
But to someone living with CKD, it can mean a great deal.
Living With CKD Is Not Only About Kidney Function
Patients know this immediately. Doctors sometimes need reminding.
Kidney disease enters daily life quietly. Through fatigue. Through swelling. Through blood pressure readings that suddenly matter more than they used to. Through routine blood work that starts to shape family conversations.
Families adjust in stages.
First by minimizing.
Then by reading.
Then by reorganizing.
That is why a good article or a good consultation should do more than explain the biology. It should help patients understand where they stand, what still matters, and what is still under their control.
That is often more useful than optimism.
FAQs on Chronic Kidney Disease Stem Cell and Exosome Therapy

Can stem cell therapy cure CKD?
No, that is not the right way to talk about it.
If a patient asks me this directly, I would say the goal is not cure. The more realistic question is whether a regenerative approach may help protect remaining kidney function in a selected case, alongside proper nephrology care.
Can damaged kidneys recover at all?
Sometimes partly, yes.
But that depends very much on what caused the damage and how much scarring is already there. Once fibrosis becomes dominant, recovery becomes much harder. That is why timing matters so much in kidney disease.
Is stem cell therapy already a standard treatment?
No.
Standard CKD treatment is still built around proven medical management, close follow-up, blood pressure control, diabetes treatment, and reduction of kidney stress where possible. That is still the main road.
Does stage 3 CKD still leave room for action?
Very often, yes.
Stage 3 is usually not the end of the story. In many patients, there is still meaningful room to slow progression, especially if the main drivers are identified and taken seriously.
Why is diabetic kidney disease discussed so often in this context?
Because it is one of the clearest CKD patterns we see.
Diabetes affects the kidney through more than one mechanism at once. Vascular injury, inflammatory stress, metabolic strain, fibrosis — they tend to come together. That is one reason this subgroup gets so much attention in regenerative medicine research.
Conclusion
Stem cell and exosome therapy for chronic kidney disease deserves a place in serious medical discussion.
Not because all the answers are already there.
And not because standard nephrology has become less important.
It deserves attention because CKD is a disease of continuing injury. Inflammation persists. Scarring advances. And in earlier or better-selected patients, there may still be room to influence some of that process before too much function has been lost.
- Patients deserve honesty here.
- They deserve more than slogans.
- More than novelty.
- More than borrowed hope.
- They deserve a careful diagnosis, a realistic timeline, proper kidney care, and a physician who can say both yes and no when needed.
- That is how this topic should be approached.
Not with hype.
With judgment.





