Some conditions do not announce themselves loudly. Avascular necrosis is one of them.
Bioplasty and Stem Cell Therapy as a Joint-Preserving Approach
Clinical Insights by Op. Dr. Hilmi Karadeniz
Orthopedic Surgeon & Sports Medicine Physician
A Personal Introduction
A sports orthopedic surgeon perspective on recovery
I am Op. Dr. Hilmi Karadeniz, an orthopedic surgeon and sports medicine physician with many years of experience treating joint and bone conditions. In my clinical practice, I work with patients whose mobility, independence, and long-term joint health depend on careful timing and well-considered treatment decisions.
Femoral head avascular necrosis is one of those conditions where understanding the disease process early can make a decisive difference.
Table of Contents
Avascular necrosis is not a sudden disease
It is a slow failure of circulation
When patients first hear the diagnosis “femoral head avascular necrosis”, they often imagine something acute. A sudden collapse. A dramatic injury. A clear moment when everything went wrong.
That is rarely how this condition actually begins.
In most cases, avascular necrosis develops quietly. Blood supply to the bone is reduced, not eliminated overnight. The femoral head continues to carry load. It continues to move. It often continues to look acceptable on early imaging. But inside the bone, the balance between survival and collapse is already shifting.
Bone tissue is alive. It depends on microcirculation.
When that circulation weakens, bone does not fail immediately – it weakens first.
This distinction matters. Because once collapse occurs, our options narrow dramatically.
My work as an orthopedic surgeon has taught me one central lesson about avascular necrosis:
Timing matters more than force.
Understanding femoral head avascular necrosis in daily practice
From a medical standpoint, avascular necrosis is often explained in one sentence: bone tissue dies because blood supply is impaired.
That sentence is correct. But it does not describe what I see in the consultation room.
What I see are patients who can still walk. Patients who still go to work. Patients who are often told that they are “not bad enough yet” for serious intervention.
They are not wrong — but the disease does not wait for permission.
The femoral head is unforgiving. Its blood supply is limited. Once that supply is compromised, the bone survives on reserve. For a while, that reserve is enough. Then it is not.
Why the femoral head is especially vulnerable
The hip joint carries enormous load. Every step concentrates force through a relatively small surface. Under normal circumstances, bone adapts constantly. It remodels. It responds.
But remodeling requires blood flow.
When circulation drops – due to corticosteroids, alcohol, trauma, systemic disease, or sometimes no identifiable cause – the femoral head loses its ability to adapt.
The bone does not break.
It starves.
And starving bone behaves differently than injured bone.
Symptoms are often misleading
One of the most difficult aspects of femoral head avascular necrosis is that pain is a late signal.
Early on, patients describe stiffness. Fatigue. A vague discomfort deep in the groin. Some days are better than others.
This variability creates false reassurance.
I have seen patients with advanced necrosis who told me:
“It doesn’t hurt that much.”
Pain is not the disease.
Pain is a consequence – and often a delayed one.
Surgery is effective – but not always the first answer
Hip replacement is one of the most successful procedures in orthopedics. When the joint has failed, it restores function reliably.
But replacing a hip is not a neutral decision, especially in younger patients.
Prostheses have a lifespan. Revisions are more complex. And once the joint is replaced, biology is no longer part of the equation.
Joint preservation exists because sometimes the joint is not yet lost.
The question is not whether we can replace the hip – the question is whether we have time not to.
Bioplasty: supporting structure, not forcing healing
Bioplasty is often misunderstood.
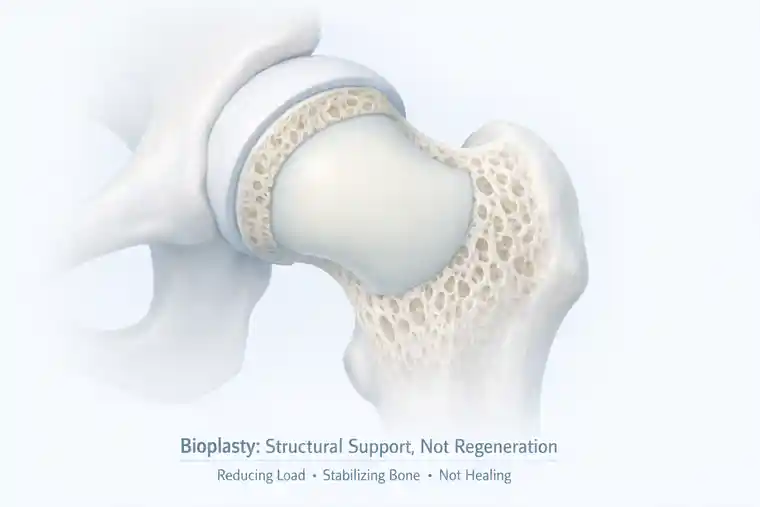
- It does not regenerate bone.
- It does not restore circulation.
- Its role is more modest – and more honest.
Bioplasty supports weakened bone. It reduces stress. It helps prevent collapse while the underlying biology is given a chance to recover.
But structure alone is not enough.
Bone does not heal because it is supported.
Bone heals because it is fed.
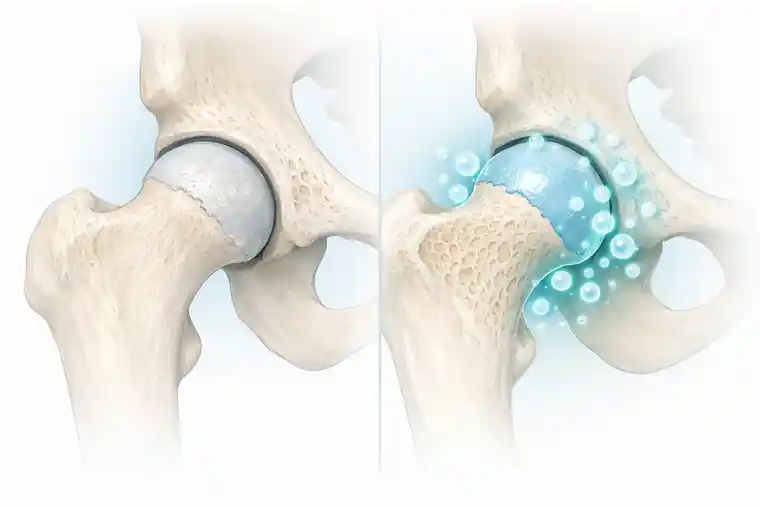
Why stem cell and exosome therapy enters the discussion
Stem cell and exosome therapy in avascular necrosis is not about replacement. It is about activation.
The goal is not to build new bone from scratch. The goal is to help the body reorganize a repair process that has failed due to poor circulation.
For this purpose, autologous adipose-derived stem cells, obtained through SVF therapy, are particularly relevant.
They do not command healing.
They influence conditions.
SVF therapy and the importance of circulation
Subcutaneous fat tissue is rich in regenerative cells. When processed appropriately, SVF contains a complex mixture of cells that support angiogenesis, inflammation modulation, and tissue signaling.
What matters in avascular necrosis is not the number of stem cells – it is what they encourage the tissue to do.
They support the formation of new microvessels. They help improve local blood flow. They create a more favorable environment for bone metabolism.
This is not fast medicine.
It is quiet medicine.
MAC (Bone Marrow–Derived Cells) and the Role of Bone-Based Regeneration
In some cases, improving the environment around the bone is not enough. When avascular necrosis affects the femoral head, the problem is not only circulation. It is also structure.
Bone is a living tissue, but it is different from muscle or tendon. It carries weight. It absorbs force. It maintains shape under constant load. When bone begins to fail, support must come from a source that understands bone.
This is where MAC – mononuclear cells obtained from bone marrow aspirate – enters the discussion. Bone marrow is not just a factory for blood cells. It is also a reservoir of progenitor cells that are naturally involved in bone maintenance and repair.
When processed appropriately, Bone Marrow Aspirate Concentrate (BMAC) contains cells that are more closely aligned with bone metabolism than those derived from fat tissue.
These cells do not rebuild bone instantly.
They do not replace collapsed structures.
What they do is more subtle.
- They participate in signaling pathways that support bone remodeling.
- They influence how bone responds to stress, injury, and reduced blood supply.
- They contribute to an environment where structural repair becomes biologically possible.
In avascular necrosis, this distinction matters.
- Adipose-derived cells primarily support circulation and inflammatory balance.
- Bone marrow–derived cells add a different layer – one that is more directly connected to bone integrity itself.
This is not about choosing one cell source over another. It is about understanding what the tissue needs. When circulation is compromised and bone structure is under threat, bone-based cellular support can be a relevant part of a joint-preserving strategy.
Again, this is not aggressive medicine. It is not fast. It does not force outcomes. It works quietly, alongside mechanical support and load reduction, to give the bone a better chance to stabilize before collapse occurs.
Why results take time – and why that is normal
Patients often ask when they will feel better.
The honest answer is: when biology allows it.
Bone does not regenerate on a schedule. Imaging changes lag behind symptoms. Symptoms fluctuate.
Improvement, when it comes, is often gradual. Less pain after daily activity. More tolerance to load. Fewer bad days.
This is not dramatic. It is durable.
Timing defines everything
- Stem cell–supported bioplasty is most effective before collapse.
- Once the femoral head loses its shape, no biological therapy can restore geometry.
- That is why patient selection matters more than technique.
- Offering regenerative therapy too late creates false hope.
- Offering it too early creates unrealistic expectations.
- The window is narrow – but real.
Recovery is an active process
This is often underestimated.
Stem cell therapy does not mean “use the joint normally.”
It means the opposite.
Load must be reduced. Movement must be controlled. Rehabilitation must respect healing timelines.
Cells cannot argue with physics.
Patients who rush recovery often lose the benefit they hoped for.
How this differs from pain-based treatment
Painkillers reduce symptoms.
They do not change the disease.
Corticosteroid injections may calm inflammation temporarily. They do not restore circulation. In some cases, they contribute to the problem.
Regenerative approaches aim to change trajectory, not comfort alone.
That distinction matters.
What patients should realistically expect
I do not promise avoidance of surgery.
I promise careful assessment.
Stem cell–supported bioplasty may slow progression. It may preserve the joint. It may delay replacement for years.
Or it may not.
Medicine is not certainty.
It is probability, timing, and responsibility.
Ethical responsibility in regenerative orthopedics
- Regenerative medicine attracts attention because it sounds powerful.
- That power requires restraint.
- Using biology to support healing is legitimate.
- Using it to sell certainty is not.
Closing thoughts
Femoral head avascular necrosis is a condition that rewards patience and punishes delay.
Bioplasty combined with autologous stem cell therapy is not a miracle. It is a joint-preserving attempt, used early, followed carefully, and explained honestly.
When it works, it does not create something extraordinary.
It preserves something ordinary.
And that, in medicine, is often the greatest success.
Additional Clinical Reflections from Practice
Over the years, I have learned that femoral head avascular necrosis teaches patience in a way few other orthopedic conditions do.
Not patience in the sense of waiting passively, but patience in listening — to symptoms, to imaging, to what the bone is quietly telling us over time.
Some patients improve more than expected.
Others stabilize without dramatic change.
A few progress despite everything being done “right.”
This variability is uncomfortable for patients and physicians alike. Modern medicine prefers predictability. Avascular necrosis offers very little of it.
What it does offer is a chance to observe biology in slow motion.
Conversations That Repeat Themselves
There are certain sentences I hear again and again.
“Doctor, I feel better, does that mean it’s healing?”
“Can I start walking normally now?”
“If I’m careful, can I avoid surgery forever?”
These questions are never unreasonable. They are human.
And the answers are rarely simple.
Feeling better does not always mean healing. Sometimes it means inflammation has settled. Sometimes it means load has shifted. Sometimes it means the body is compensating.
True healing in bone takes time – often longer than patience allows.
Why Imaging and Symptoms Must Be Read Together
One of the mistakes I see frequently is relying too heavily on either symptoms or imaging alone.
- An MRI can look alarming while the patient feels relatively well.
- A patient can feel comfortable while imaging quietly worsens.
- Neither tells the full story on its own.
In femoral head avascular necrosis, progress is best judged over time, not at a single moment. Patterns matter more than snapshots.
This is why follow-up, consistency, and honest reassessment are so important.
The Psychological Weight of “Waiting”
Waiting is not neutral.
For many patients, the period after diagnosis but before a definitive outcome is emotionally exhausting. They are asked to protect a joint that still feels usable. They are asked to limit activity while still living their lives.
This is harder than it sounds.
Some patients follow recommendations precisely. Others struggle. Not because they are careless, but because life does not pause for biology.
Understanding this helps me be more realistic — and more forgiving — when outcomes are not perfect.
When Progress Is Quiet but Meaningful
Success in joint-preserving treatment is rarely dramatic.
It often looks like:
- pain that no longer escalates
- imaging that remains stable
- activity that becomes predictable again
- fewer bad days
These are not outcomes that make headlines.
But for patients, they matter deeply.
Delaying joint replacement by five or ten years can change the trajectory of a life.
The Role of Trust in Long-Term Management
- Managing avascular necrosis is not a single decision. It is a relationship.
- Patients need to trust that recommendations are not arbitrary.
- Physicians need to trust that patients are doing their best.
- When that trust exists, outcomes – even imperfect ones – are easier to accept.
- When it doesn’t, frustration grows quickly.
Accepting Limits Without Losing Hope
One of the most difficult parts of my job is telling patients that biology has limits.
Stem cell–supported bioplasty is not a promise. It is an attempt.
Sometimes a successful one. Sometimes not enough.
Accepting that reality does not mean giving up hope.
It means replacing illusion with clarity.
And clarity, in medicine, is a form of respect.
Why Joint Preservation Is Still Worth Discussing
Even knowing the limits, I continue to discuss joint-preserving options with appropriate patients.
Not because they always work — but because when they do, they offer something no prosthesis can:
time with one’s own joint.
That time may be measured in years, not decades. But for many patients, those years matter.
When progress is quiet
Femoral head avascular necrosis reminds us that not all progress is visible and not all success is dramatic.
- Sometimes the best outcome is stability.
- Sometimes it is delay.
- Sometimes it is simply avoiding deterioration while life continues.
- Bioplasty combined with autologous stem cell therapy belongs in that space – between action and restraint, between intervention and respect for biology.
When used thoughtfully, it does not promise miracles.
It offers a chance.
And in many cases, that chance is enough.
Long-Form Reflection: Making Decisions When Certainty Does Not Exist
One of the quiet truths about femoral head avascular necrosis is that it rarely offers clear answers at the moment decisions must be made.
Patients often expect medicine to work like mathematics: if the diagnosis is clear, the solution should be clear as well. In reality, this condition lives in the space between probabilities, not certainties.
I am often asked, “What would you do if this were your hip?” It is a reasonable question.
It is also a difficult one.
Because what I would do depends on timing, tolerance for risk, lifestyle, and how much uncertainty I am willing to live with. And those variables are different for every person who sits across from me.
There is a particular kind of discomfort that comes with recommending a joint-preserving approach.
If the joint were already destroyed, the decision would be simple. Replace it. Restore function. Move forward.
But when the joint is not yet lost, every option carries a trade-off.
Intervening early means acting before collapse — but also before outcomes can be predicted with confidence. Waiting preserves the option of surgery later, but risks losing the window where preservation was still possible.
- Neither path is wrong.
- Neither path is guaranteed.
- This is where medicine stops being technical and becomes personal.
- In these moments, I try to slow the conversation down.
- Not to delay action, but to allow space for understanding what is actually being decided.
We are not deciding whether stem cells “work” or whether bioplasty is “better” than surgery. We are deciding how much uncertainty a person is willing to carry, and for how long.
Some patients are comfortable with that uncertainty. They understand that stabilization, not cure, may be the best outcome. They are willing to protect the joint, adjust their activity, and accept gradual change.
Others are not. They want clarity, predictability, a defined endpoint.
Both positions are valid.
What complicates this further is that avascular necrosis does not progress at the same pace in everyone.
- I have seen patients remain stable for years with minimal intervention.
- I have seen others progress rapidly despite careful management.
- There is no single variable that explains this completely. Biology, load, vascular reserve, systemic factors – all play a role, and none can be isolated cleanly.
This unpredictability makes protocol-driven medicine uncomfortable.
It also makes honest conversation essential.
When discussing stem cell–supported bioplasty, I am careful not to frame it as a solution, but as a direction.
A direction toward preservation rather than replacement.
A direction toward supporting biology rather than bypassing it.
But directions can change.
And patients need to know that choosing a joint-preserving path does not lock them into it forever. Surgery remains an option if the disease progresses. Choosing preservation first does not mean refusing surgery later.
That flexibility often reduces anxiety.
Another aspect of uncertainty that is rarely discussed openly is the emotional burden on the physician.
Making recommendations when outcomes cannot be guaranteed requires humility. It requires acknowledging limits – not just of treatment, but of prediction.
There are moments when I revisit decisions months or years later and ask myself whether a different recommendation would have changed the outcome.
Sometimes the answer is yes.
Often, it is no.
But the question itself is part of practicing responsibly.
I have learned that patients often handle uncertainty better than we expect — when it is explained honestly.
What they struggle with is ambiguity presented as confidence.
Saying “this will fix it” may feel reassuring in the moment, but it undermines trust when reality unfolds differently. Saying “this may help, and here is what that help realistically looks like” is harder, but more sustainable.
In the long run, clarity without certainty builds stronger partnerships.
Decision-making in avascular necrosis is rarely about choosing the “best” option.
It is about choosing the most appropriate option at this moment, knowing that the situation may evolve.
That evolution does not mean failure.
It means adaptation.
Just as bone adapts – or fails to – under changing conditions, treatment strategies must remain flexible.
Perhaps the most important realization I have come to is this:
- Choosing a joint-preserving approach is not a commitment to optimism.
- It is a commitment to attentiveness.
- It requires regular reassessment.
- It requires listening to symptoms without overreacting to them.
- It requires accepting that stability is sometimes the best achievable outcome.
For patients who understand and accept this, regenerative strategies can make sense. For those who need certainty and closure, earlier surgical intervention may be the kinder choice.
- There is no failure in choosing surgery.
- There is no virtue in avoiding it at all costs.
- The only real mistake is ignoring biology – or ignoring the person living with it.
- In femoral head avascular necrosis, uncertainty is not a flaw in medicine.
It is part of the condition itself.
Our responsibility is not to eliminate that uncertainty, but to navigate it honestly, thoughtfully, and together with the patient.
When decisions are made that way, even imperfect outcomes remain acceptable — because they were chosen with clarity, not illusion.
FAQ’s regarding Femoral Head Avascular Necrosis
Can femoral head avascular necrosis heal on its own, without surgery?
This is usually asked very quietly. And I understand why.
The word necrosis sounds final. It sounds like something that only moves in one direction. In reality, the situation is more nuanced.
In very early stages, before the femoral head has lost its shape, the condition can sometimes stabilize. Not because the bone magically heals itself, but because the circulation problem does not always progress at the same speed in everyone.
Once collapse has started, however, the bone cannot simply recover on its own. At that point, we are no longer talking about healing, but about managing damage.
So the honest answer is not yes or no.
It is when, how far, and what the bone is still capable of.
Does stem cell therapy really work for avascular necrosis?
This question usually comes after patients have read a lot online — and feel more confused than informed.
Stem cell therapy does not work in the way many people imagine. It does not replace dead bone. It does not rebuild a collapsed joint.
What it can sometimes do is support the conditions the bone needs in order to survive longer. Especially circulation. Especially in earlier stages.
In other words, it may help the bone cope better — not become something new.
For some patients, that difference is meaningful.
For others, it is not enough.
Both outcomes exist, and pretending otherwise would not be honest.
If I feel less pain after treatment, does that mean the disease is gone?
This is an important question – and a dangerous assumption.
Pain is only one signal, and often not the most reliable one in avascular necrosis. Some patients feel better while the bone is still fragile. Others feel pain even when the situation is relatively stable.
Feeling better does not automatically mean healing. Sometimes it means inflammation has calmed down. Sometimes it means the body has adapted.
This is why follow-up imaging and time matter more than a single good or bad week.
In this condition, less pain is encouraging — but never the full story.
How long does recovery take if I choose a joint-preserving treatment?
Most people hope the answer will be measured in weeks.
It usually isn’t.
Bone responds slowly. Blood vessels grow slowly. Adaptation takes time. Even when everything goes well, progress tends to be gradual.
Some patients notice changes after a few months. Others need much longer before things feel stable. And during that time, activity often has to be limited more than patients expect.
Recovery here is not about getting back to normal quickly.
It is about not making things worse while biology does its work.
Can stem cell treatment help me avoid a hip replacement completely?
This is often the real question behind all the others.
And the most honest answer is this: sometimes yes, sometimes no.
In patients diagnosed early, before collapse, stem cell–supported approaches may delay or even prevent the need for a hip replacement. In other cases, they simply buy time.
Once the femoral head has collapsed, avoiding surgery becomes unlikely, no matter what treatment is used.
The goal is not to promise avoidance of surgery.
The goal is to make decisions at the right moment, not too early and not too late.





